Camelia Ciobanu, MD1, Amr Dokmak, MD1, Arnold Forlemu, MD1, Manasa Ginjupalli, MD1, Madhavi Reddy, MD2 1Brooklyn Hospital Center, Brooklyn, NY; 2The Brooklyn Hospital Center, Brooklyn, NY Introduction: Sarcoidosis is a chronic, multisystem granulomatous disease that rarely involves the gastrointestinal (GI) tract and liver. Gastric sarcoidosis is typically asymptomatic, with only 0.1–0.9% of patients exhibiting symptoms. Hepatic involvement is more common, occurring in approximately 11.5% of cases, although only 5–15% are symptomatic. We present a rare case of sarcoidosis initially manifesting with GI symptoms and weight loss, without pulmonary involvement.
Case Description/
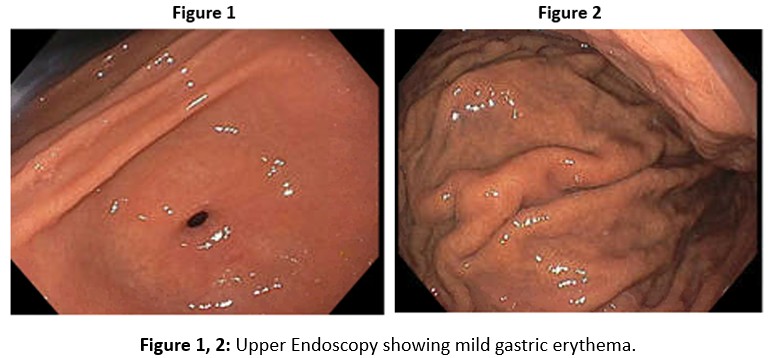
Methods: A 42-year-old male with a history of hyperlipidemia and vitamin D deficiency presented with abdominal pain, alternating bowel habits, 20-pound weight loss, and imaging revealing lymphadenopathy. Physical examination showed enlarged cervical and axillary lymph nodes. Laboratory evaluation revealed elevated alkaline phosphatase (ALP 159 U/L) with normal AST, ALT, and bilirubin. CT imaging demonstrated extensive mediastinal and abdominal lymphadenopathy, along with terminal ileum and cecal wall thickening. Stool studies and celiac panel were unremarkable. Esophagogastroduodenoscopy (EGD) revealed mild gastric erythema (Figure 1, 2); biopsies showed mild chronic inflammation and focal non-caseating granulomas (Figure 3). Colonoscopy revealed benign polyps with no granulomas or mucosal abnormalities. A comprehensive workup for chronic liver disease, including viral, autoimmune, and metabolic causes, was negative except for a positive ANA (1:80), elevated IgG (2129 mg/dL), and an elevated ACE level (99 U/L). ALP isoenzyme analysis confirmed hepatic origin. Vitamin D was severely deficient. Based on serologic, histologic and imaging findings, a diagnosis of sarcoidosis with gastric and hepatic involvement was made. The patient was started on prednisone 20 mg daily and pantoprazole. Close outpatient follow-up was arranged to monitor symptoms and liver function. Discussion: This case highlights the diagnostic challenge of extrapulmonary sarcoidosis presenting with isolated GI and hepatic involvement. Early recognition is essential for appropriate management. Due to the absence of standardized guidelines, treatment remains individualized, with corticosteroids serving as the cornerstone for symptomatic disease.
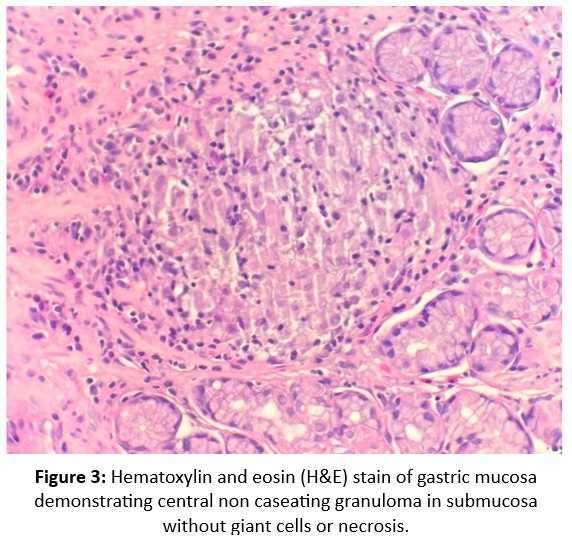
Figure: Hematoxylin and eosin (H&E) stain of gastric mucosa demonstrating central non caseating granuloma in submucosa without giant cells or necrosis.
Disclosures: Camelia Ciobanu indicated no relevant financial relationships. Amr Dokmak indicated no relevant financial relationships. Arnold Forlemu indicated no relevant financial relationships. Manasa Ginjupalli indicated no relevant financial relationships. Madhavi Reddy indicated no relevant financial relationships.
Camelia Ciobanu, MD1, Amr Dokmak, MD1, Arnold Forlemu, MD1, Manasa Ginjupalli, MD1, Madhavi Reddy, MD2. P3876 - Silent Lungs, Symptomatic Gut: Atypical Sarcoidosis Presenting With Gastrointestinal and Hepatic Manifestations, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")