Department of Internal Medicine, Texas Health Presbyterian Hospital Dallas, Texas Health Resources, Dallas, TX Dallas, TX
Bryan Hoang, MD, Samantha Lujan, MD, Rita Lepe, MD Texas Health Dallas, Dallas, TX Introduction: Tocilizumab, an interleukin-6 (Il-6) receptor inhibitor, is used to treat a variety of rheumatologic conditions including rheumatoid arthritis (RA). It is typically administered via IV infusion over 60 minutes; faster infusion is discouraged due to risk of hypersensitivity reactions. Though uncommon, serious GI complications such as bowel ischemia, pneumatosis, and perforation have been reported. We present a case of multiorgan failure with gastrointestinal and hepatic involvement following rapid tocilizumab infusion in a patient with underlying primary biliary cholangitis (PBC).
Case Description/
Methods: A 62-year-old woman with RA and cirrhosis from PBC presented with progressive bilateral lower extremity weakness, diarrhea, and falls. She had been receiving monthly tocilizumab infusions but, four days prior to presentation, received her usual dose over 20 minutes instead of the recommended 60. Baseline liver function and INR were normal. On admission, she was found to have AST 846 U/L, ALT 273 U/L, bilirubin 9.3 mg/dL, and INR 1.5. Her condition worsened with progressive encephalopathy, hyperbilirubinemia (peak 10.6 mg/dL), worsening transaminases, and INR peaked to 3.5. Computed tomography (CT) imaging revealed extensive bowel pneumatosis, but no perforation. Eventually the patient developed hypoxic respiratory failure, renal failure, and shock requiring intensive care unit (ICU) level care. Discussion: Gastrointestinal (GI) manifestations in this case were prominent and may have been mediated by tocilizumab impairing gut barrier function through Il-6 inhibition. Il-6 promotes vascular endothelial growth factor (VEGF) signaling to maintain mucosal blood flow and epithelial repair via nitric oxide and prostaglandin production; thus, its inhibition may impair intestinal perfusion and increase the risk of ischemia. This is a rare case suggesting that rapid infusion may amplify endothelial dysfunction that eventually led to bowel pneumatosis, acute liver failure, and subsequently multiorgan failure. While faster infusion protocols have been deemed safe in select populations without significant comorbidities, their safety in patients with cirrhosis remains uncertain. Hence the patient's underlying cirrhosis likely increased her susceptibility to ischemic gut injury and hepatic decompensation. This case highlights the need for caution and prompt recognition of early organ injury in high-risk patients receiving tocilizumab, particularly in the context of rapid infusion.
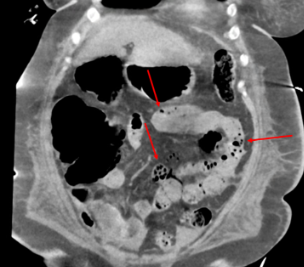
Figure: Coronal CT abdomen and pelvis without contrast: Extensive small bowel pneumatosis (red arrows).
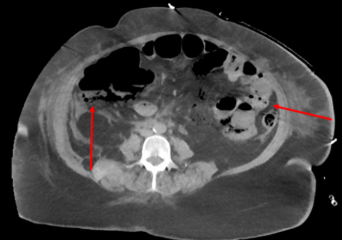
Figure: Axial CT abdomen and pelvis without contrast: Colon pneumatosis (red arrows)
Disclosures: Bryan Hoang indicated no relevant financial relationships. Samantha Lujan indicated no relevant financial relationships. Rita Lepe indicated no relevant financial relationships.
Bryan Hoang, MD, Samantha Lujan, MD, Rita Lepe, MD. P3849 - Tocilizumab-Induced Multiorgan Failure Following Rapid Infusion: A Case of Acute Liver Failure and Bowel Pneumatosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")