Eitan Scheinthal, DO1, Nishkarsh Kumar, 2, Darly Knoedler, MD3, Sahibzada Usman Latif, MD1 1Aurora Healthcare, Milwaukee, WI; 2St. Luke's Hospital, Milwaukee, WI; 3Great Lakes Pathology, Milwaukee, WI Introduction: Sclerosing epithelioid mesenchymal neoplasm (SEMN) is a recently described pancreatic tumor with few reported cases in the literature. It is characterized by its molecular markers and histologic features that distinguish it from other pancreatic neoplasms. Its natural history typically follows an indolent course and prognosis is favorable following surgical resection.
Case Description/
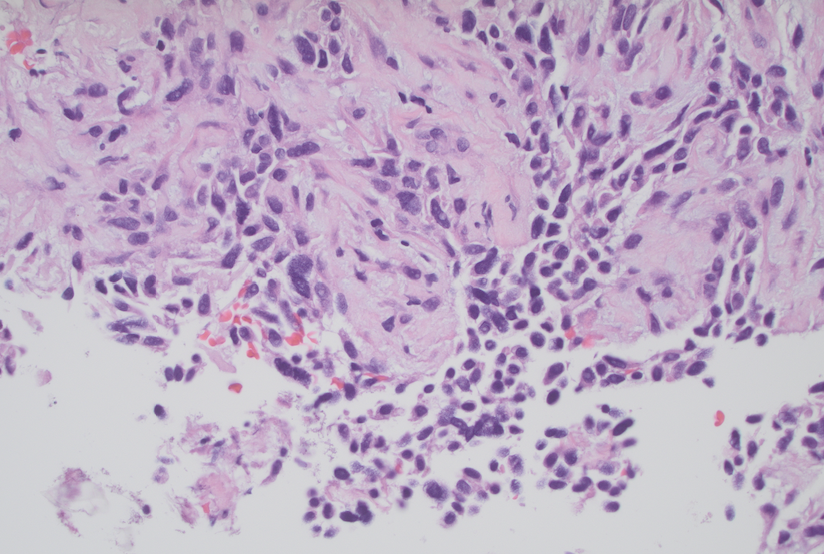
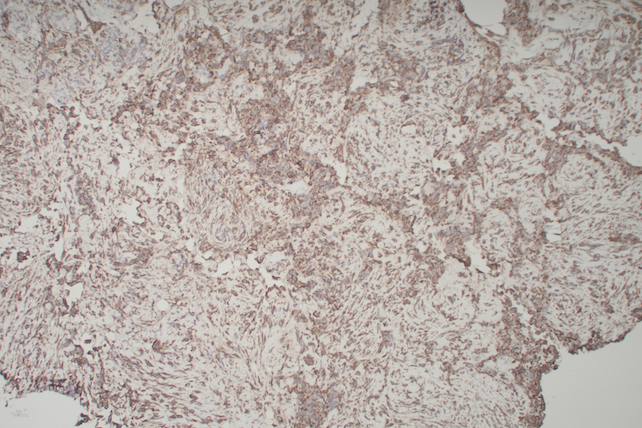
Methods: A 57-year old male was referred to our clinic for abnormal liver enzymes and painless jaundice. He reported an 80lb unintentional weight loss over 24 months along with more recent tan-colored stools, progressive jaundice and scleral icterus. He denied family history of gastrointestinal malignancy, alcohol use and herbal supplement use. He endorsed tobacco use. Labs showed T Bili 10.1 mg/dL, AST 116 U/L, ALT 336 U/L, ALP 355 U/L, CA 19-9 22 U/mL, CEA < 2 ng/mL, AFP < 3 ng/mL. On CT a 28mm pancreatic lesion was seen, stable from prior that was identified in retrospect. There were no other lesions. MRI MRCP showed a round, indistinct and T2 hyperintense 25 mm pancreatic head mass. The pancreatic duct was normal. The common bile duct (CBD) was mildly dilated with caliber change at the intrapancreatic portion. EUS/ERCP confirmed the mass and distal CBD stricture. Biliary decompression was performed with biliary sphincterotomy and a 10 mm x 6 cm uncovered biliary metal stent was deployed. EUS guided FNB was pursued. Cytology showed numerous neoplastic epithelioid cells with fragments of spindle cell parenchyma and cells arranged into poorly preserved, irregularly shaped nests. Immunohistochemistry was positive for Pancytokeratin, Vimentin, E-cadherin, CD10 and weakly positive for Moc 3 (Figures 1, 2). It was negative for ß-catenin (nuclear), CD34 and S-100P. A diagnosis of pancreatic sclerosing epithelioid mesenchymal neoplasm was made. Discussion: Presently little is known about pancreatic SEMN and its clinical course. It primarily affects young females and has a predilection for growth in the pancreatic head. We present the case of a middle-aged male with a pancreatic head SEMN causing painless obstructive jaundice. Its stability on imaging contributed to a 31-month delay in diagnosis. The clinical course has been described as indolent, but here was slowly progressive. While rare, it should be considered on the differential diagnosis of solitary pancreatic neoplasms. Staining for Vimentin and CD99 should be requested. This case expands the medical literature on SEMN demographics, diagnosis and natural history.
Figure: Figure 1. H and E-High power view (400x) of epitheloid and spindle cells
Figure: Figure 2. Vimentin immunostain-Epitheloid and stromal cells both positive, associated normal pancreatic acinar tissue negative
Disclosures: Eitan Scheinthal indicated no relevant financial relationships. Nishkarsh Kumar indicated no relevant financial relationships. Darly Knoedler indicated no relevant financial relationships. Sahibzada Usman Latif indicated no relevant financial relationships.
Eitan Scheinthal, DO1, Nishkarsh Kumar, 2, Darly Knoedler, MD3, Sahibzada Usman Latif, MD1. P4424 - Sclerosing Epithelioid Mesenchymal Pancreatic Tumor: A Rare Case of Obstructive Jaundice, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.