Rasheed Musa, MBBS, Parth Goenka, , Asaiel Makahleh, MD, Amira Eftaiha, MD, Elizabeth Arze, MD, Puneet Goenka, MD, Mark Young, MD East Tennessee State University, Johnson City, TN Introduction: Pancreatic ductal adenocarcinoma (PDAC) is a highly aggressive malignancy, with common sites of metastasis including the liver, lungs, and peritoneum. Metastasis to the rectum is exceedingly rare and has seldom been reported in the literature. Here, we present the case of a 58-year-old male who presented with jaundice and intermittent rectal bleeding and was ultimately diagnosed with metastatic pancreatic cancer involving both the liver and rectum.
Case Description/
Methods: A 58-year-old male with a medical history of hypertension was referred to our hospital for evaluation of progressive jaundice and intermittent episodes of bleeding per rectum. On examination, the patient was icteric, with normal vital signs. No palpable abdominal or rectal masses were noted.
Laboratory evaluation revealed elevated liver enzymes in an obstructive pattern. Serum bilirubin was elevated to 5.8 mg/dL. CA 19-9 was significantly elevated at 640 U/mL, and serum CEA was within normal limits.
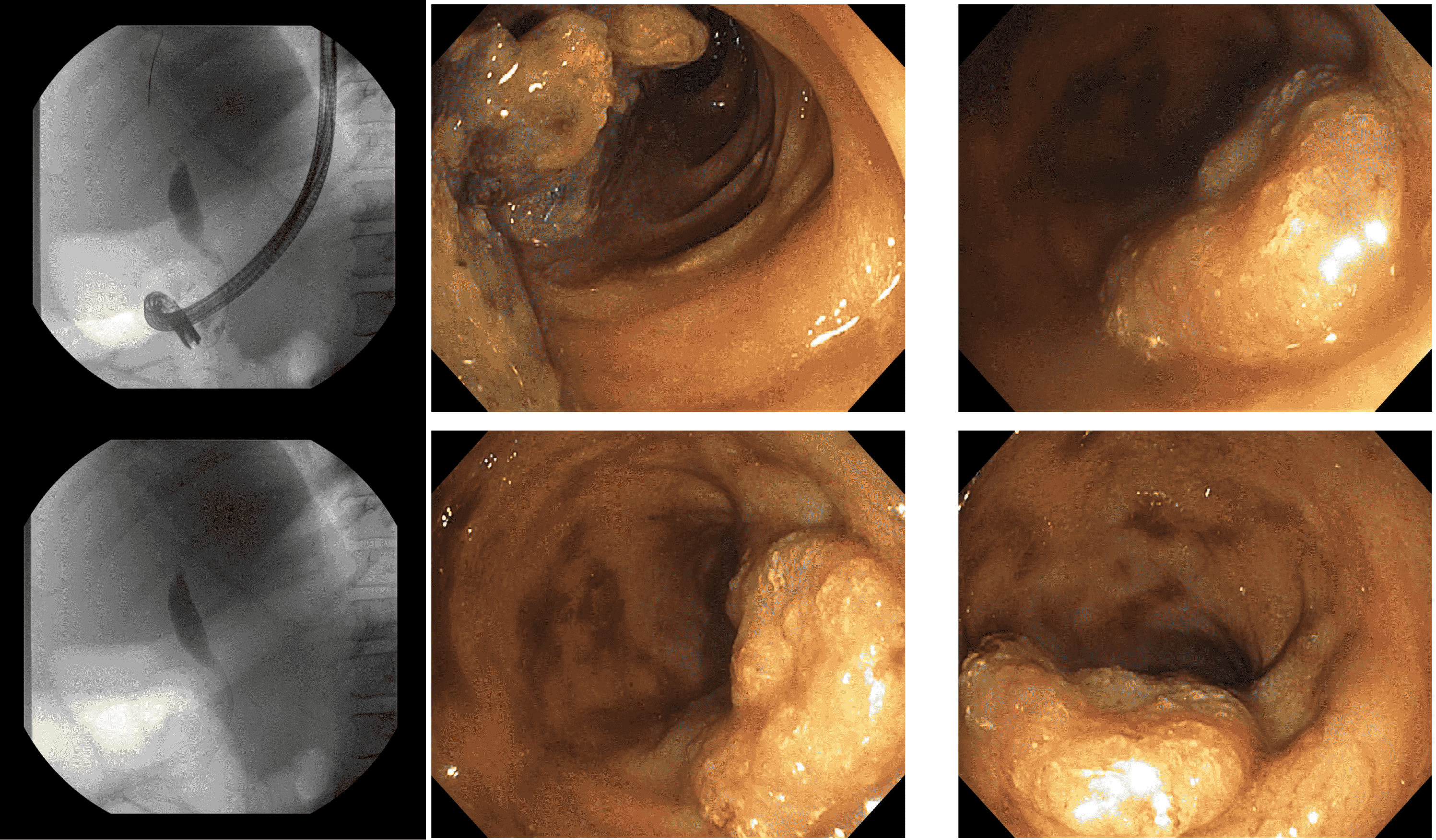
An MRI of the abdomen demonstrated a pancreatic neck mass, measuring approximately 3.2 cm, with multiple hepatic lesions suggestive of metastatic disease and biliary dilation. Endoscopic retrograde cholangiopancreatography (ERCP) was performed, which confirmed the presence of a distal biliary stricture. A biliary stent was placed, and brushings were taken for cytology.
To confirm the diagnosis, a CT-guided liver biopsy was performed, with pathology confirming poorly differentiated carcinoma consistent with pancreaticobiliary origin.
Given the patient’s complaint of intermittent rectal bleeding, a colonoscopy was performed, revealing a 4-cm friable rectal mass located 6 cm from the anal verge. Biopsies of the lesion confirm metastatic pancreaticobiliary adenocarcinoma. Discussion: Metastases to the rectum from pancreatic cancer are exceedingly rare, with only a few cases documented. The mechanism of rectal metastasis is hypothesized to involve hematogenous or lymphatic spread, although direct peritoneal seeding cannot be excluded. Presenting symptoms, including rectal bleeding, can mimic primary colorectal malignancies, underscoring the need for biopsy and histopathologic correlation to differentiate between primary and secondary tumors.
It is important to consider metastatic pancreatic cancer in the differential diagnosis of rectal masses, particularly in patients with known primary pancreaticobiliary malignancy. Early recognition of atypical metastatic patterns can guide timely diagnosis and appropriate palliative care.
Figure: Fluoroscopy and Endoscopy images
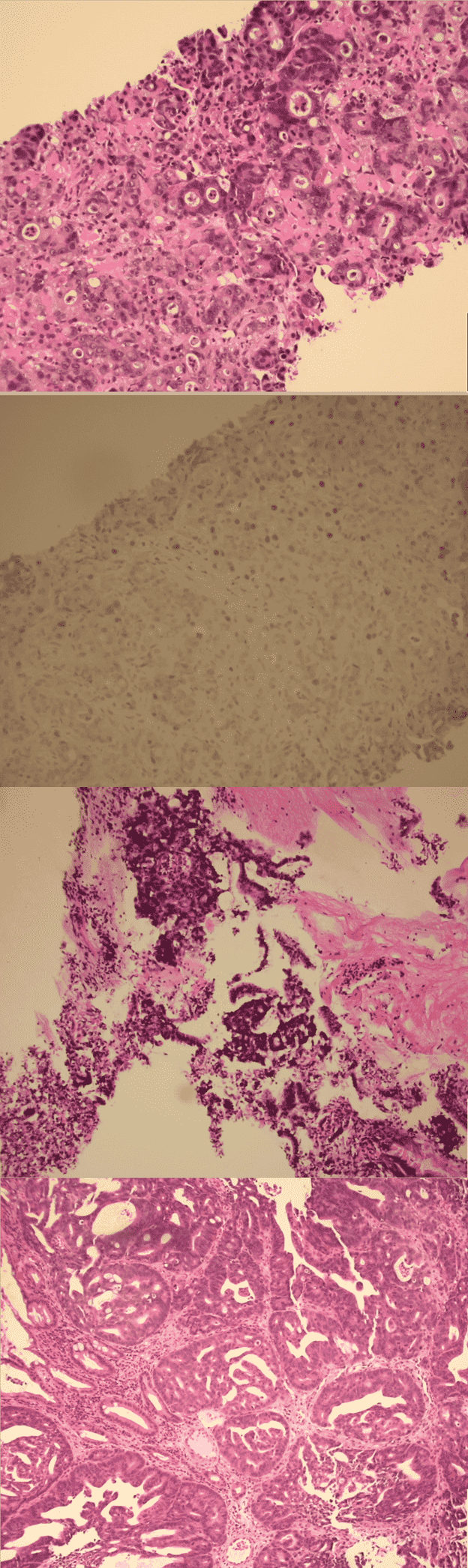
Figure: Pathology slides, respectively:
- Liver biopsy showing adenocarcinoma with gland formation
- Liver biopsy- SATB2 immunostain
- Bile Duct Stricture Brushing - adenocarcinoma
- Rectal mass biopsy - Adenocarcinoma showing cribriform pattern
Disclosures: Rasheed Musa indicated no relevant financial relationships. Parth Goenka indicated no relevant financial relationships. Asaiel Makahleh indicated no relevant financial relationships. Amira Eftaiha indicated no relevant financial relationships. Elizabeth Arze indicated no relevant financial relationships. Puneet Goenka indicated no relevant financial relationships. Mark Young indicated no relevant financial relationships.
Rasheed Musa, MBBS, Parth Goenka, , Asaiel Makahleh, MD, Amira Eftaiha, MD, Elizabeth Arze, MD, Puneet Goenka, MD, Mark Young, MD. P4413 - Dual Alarms of Metastatic Pancreatic Cancer: A Rare Case of Jaundice and Rectal Bleeding Unveiling Rectal Involvement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")