Ishan Antony, MD1, Ali Shaat, MD2, Akshay Kapoor, MD2, Ming V.. Lin, MD2 1Beth Israel Lahey Health, Burlington, MA; 2Lahey Hospital and Medical Center, Burlington, MA Introduction: Lipoprotein X (Lp-X) is an abnormal lipoprotein that accumulates in the setting of cholestasis, leading to extreme hypercholesterolemia and hyperviscosity syndrome. While Lp-X has been described in primary biliary diseases, its occurrence following liver transplantation is rare. This case highlights Lp-X in a liver transplant recipient with posttransplant anastomotic stricture and antibody-mediated rejection (AMR), and its impact on posttransplant management.
Case Description/
Methods: A 45-year-old male with decompensated cirrhosis secondary to alcohol-associated liver disease underwent a deceased donor liver transplant in March 2024. Postoperatively in April, he developed worsening cholestasis (bilirubin 21.6 mg/dL, alkaline phosphatase 1700 U/L). ERCP revealed an anastomotic stricture, which was managed with stenting. Despite stricture resolution on follow-up ERCPs in May and June, his cholestasis persisted. Liver biopsy in June demonstrated severe lobular cholestasis with feathery degeneration but no rejection. By July 2024, the patient developed progressive hypercholesterolemia (total cholesterol >1400 mg/dL, LDL >800 mg/dL) and lipid exudative retinopathy. Lipoprotein electrophoresis confirmed Lp-X as the predominant lipoprotein fraction. Given persistent cholestasis and newly detected donor-specific antibodies, AMR was suspected. He was treated with plasmapheresis, IVIG, and rituximab, leading to transient lipid reduction and vision improvement. However, hyperlipidemia persisted, contributing to symptomatic hyperviscosity syndrome, seizures, anemia, and acute kidney injury from bile cast nephropathy.Given his refractory disease and ongoing liver dysfunction, he was listed for re-transplantation. Discussion: This case underscores the need to recognize Lp-X as a severe complication of posttransplant cholestasis. Unlike primary hyperlipidemia, Lp-X is unresponsive to lipid-lowering agents, necessitating a focus on bile clearance. While plasmapheresis provides temporary relief, definitive treatment requires addressing the underlying liver dysfunction and cholestasis. The concurrent biliary anastomotic stricture and AMR leading to Lp-X accumulation in this patient represent a rare post-liver transplant complication. This appears to be the first reported case of Lipoprotein X-induced hyperlipidemia post-liver transplant in a patient without primary sclerosing cholangitis (PSC) or primary biliary cholangitis (PBC), highlighting its occurrence in non-autoimmune cholestatic liver disease.
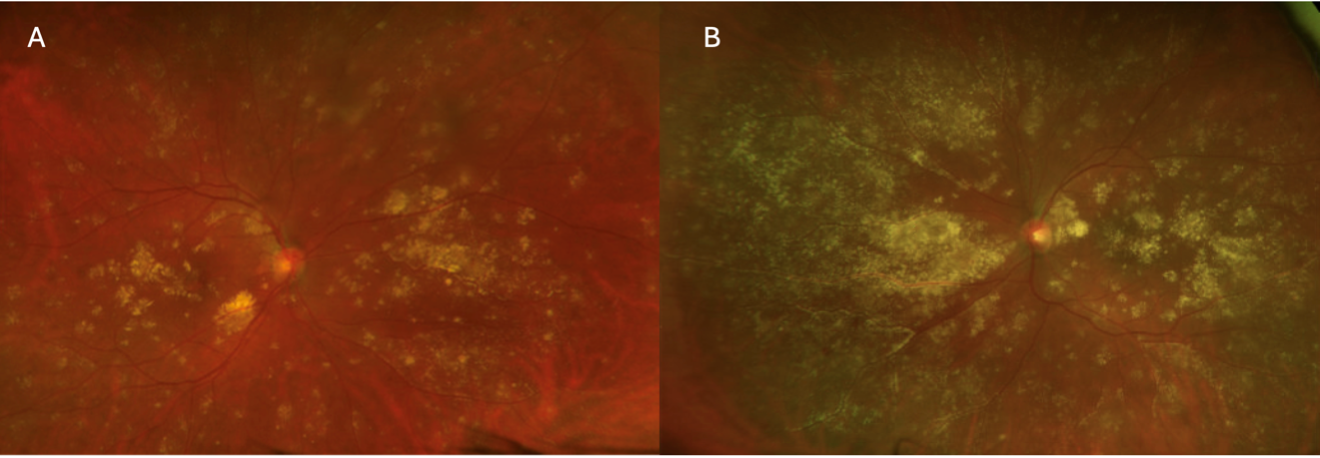
Figure: Figure 1: A) Fundoscopic image showing lipid exudative retinopathy of the right eye. B) Fundoscopic image showing lipid exudative retinopathy of the left eye.
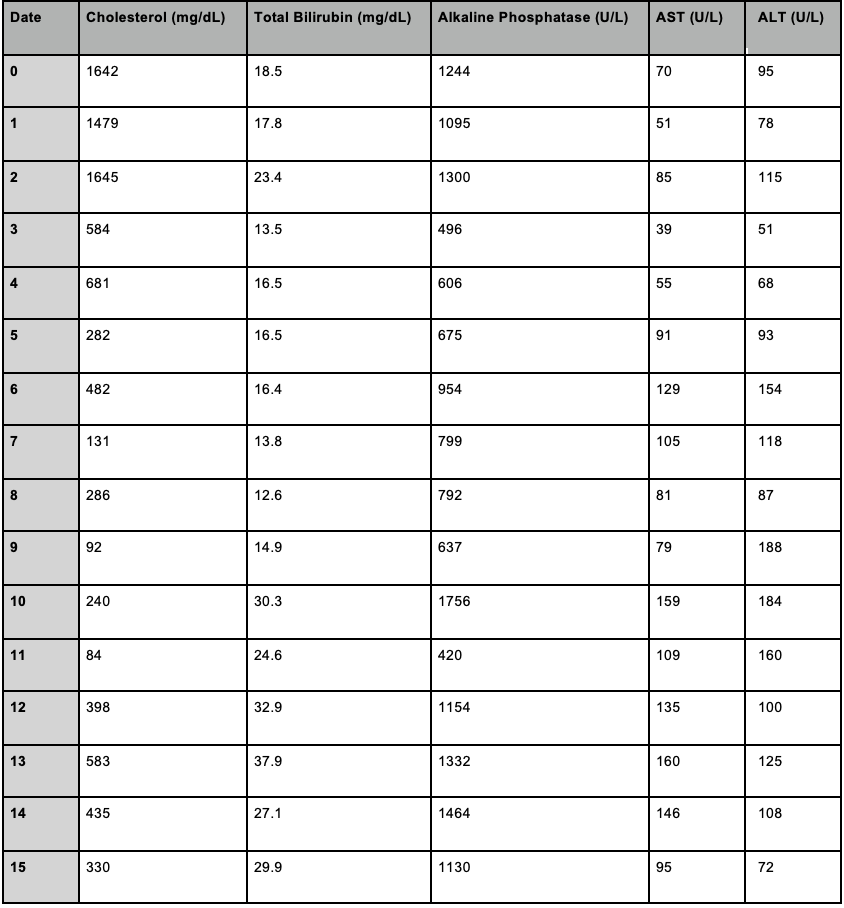
Figure: Table 1: Serial lipid profile trends before and after plasmapheresis, demonstrating transient improvement.
Disclosures: Ishan Antony indicated no relevant financial relationships. Ali Shaat indicated no relevant financial relationships. Akshay Kapoor indicated no relevant financial relationships. Ming Lin indicated no relevant financial relationships.
Ishan Antony, MD1, Ali Shaat, MD2, Akshay Kapoor, MD2, Ming V.. Lin, MD2. P4494 - Lipoprotein X-Induced Hyperlipidemia in a Liver Transplant Recipient With Cholestasis and Antibody-Mediated Rejection, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.