Rama Tarakji, MD, MPH, Mohamed Karam Douedari, MD, Neil Chokshi, DO, Hernando Gonzalez Quiros, MD, Manuel Berzosa, MD Mount Sinai Medical Center, Miami Beach, FL Introduction: Endometriosis is the presence of endometrial glands and tissue outside the uterus. Deep infiltrating endometriosis (DIE) represents less than 20% of cases. Rectal DIE is rare and often mimics malignancy. This case describes a 50-year-old female with coccygeal pain who was found to have a rectal mass consistent with rectal DIE.
Case Description/
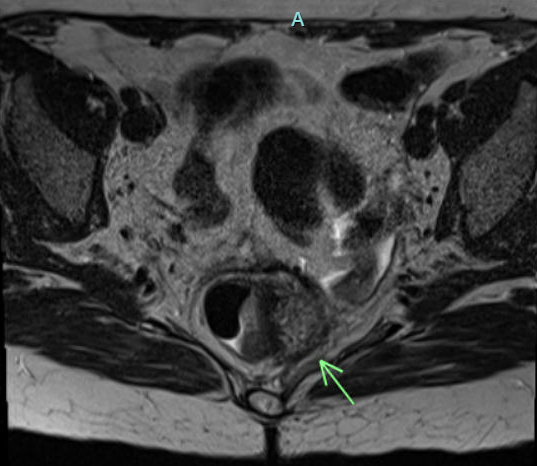
Methods: A 50-year-old woman with prior hysterectomy for vaginal prolapse and uterine bleeding, presented with persistent, intense anal and coccygeal pain. MRI showed asymmetric wall thickening of the left superior rectum, concerning for malignancy or proctocolitis. Colonoscopy with Endoscopic Ultrasound showed a heterogeneous rectal mass with poorly defined borders, partially obstructing the lumen at 7 cm from the anal verge. Sonographic features suggested invasion of the muscularis propria into perirectal fat, concerning for adenocarcinoma. Biopsies and histopathological examination confirmed rectal endometriosis. Immunohistochemical staining was positive for CD10 and PAX8, which are markers for endometrial stromal and epithelial elements. Discussion: Rectal endometriosis is a rare form of deep-infiltrating endometriosis. Diagnosis is challenging due to non-specific symptoms, such as pain and GI disturbances. It can mimic other gastrointestinal pathologies, especially malignancy. In this case, diagnosis was delayed as the patient’s chronic pain was initially attributed to uterine prolapse and managed with hysterectomy; however, her pain persisted. Imaging studies raised suspicion for a neoplastic process in the rectum. Colonoscopy and EUS revealed a rectal mass and identified the depth of the lesion but did not differentiate deep infiltrating rectal endometriosis from malignancy, as the extension into perirectal fat was highly suggestive of adenocarcinoma. Importantly, biopsy is often negative. A retrospective analysis showed that only 13.3% of cases of invasive rectal endometriosis are diagnosed via endoscopic biopsy due to the submucosal or deeper location of the endometrial tissue. In our case, definitive diagnosis was made with biopsy and immunohistochemical staining. Rectal endometriosis is an uncommon but important differential diagnosis for rectal masses in women. This case highlights the diagnostic challenge due to nonspecific rectal or pelvic symptoms and deeper tissue location, leading to negative biopsies. Increased awareness may prevent misdiagnosis and unnecessary aggressive treatments for presumed malignancy.
Figure: Image 1: MRI image showing mid-rectal asymmetric wall thickening identified in the left superior rectum, suggestive of malignancy.
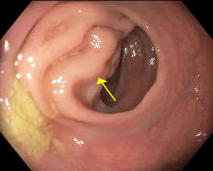
Figure: Image 2: Endoscopy picture showing a non-circumferential, non-obstructing large mass measuring 20 cm in the rectum.
Disclosures: Rama Tarakji indicated no relevant financial relationships. Mohamed Karam Douedari indicated no relevant financial relationships. Neil Chokshi indicated no relevant financial relationships. Hernando Gonzalez Quiros indicated no relevant financial relationships. Manuel Berzosa indicated no relevant financial relationships.
Rama Tarakji, MD, MPH, Mohamed Karam Douedari, MD, Neil Chokshi, DO, Hernando Gonzalez Quiros, MD, Manuel Berzosa, MD. P4609 - Beyond the Lumen: Endometriosis Invading Rectal Mucosa and Imitating Cancer, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.