
Tuesday Poster Session
Category: Colon
Nupur Savalia, MD
Scripps Mercy Hospital, CA
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma (NHL). Extranodal involvement, including within the gastrointestinal (GI) tract, occurs frequently. However, primary gastrointestinal diffuse large B-cell lymphoma (GI-DLBCL) is an exceedingly rare and aggressive form of NHL. Risk factors include infections such as Helicobacter pylori and human immunodeficiency virus, celiac disease, and inflammatory bowel disease. In clinical practice, 50% of patients are diagnosed in late stages. P</span>resentation is non-specific and may contribute to serious GI complications such as obstruction, perforation, or bleeding. We present a rare case of GI-DLBCL in a patient without known risk factors, complicated by bowel perforation. An 84-year-old male with history of diverticulosis, hemorrhoids, and asthma presented with 3 days of fevers, myalgias, urinary frequency and bilateral flank and left lower quadrant pain. One week prior, patient had two episodes of bloody diarrhea. Serum laboratory testing was significant for mild leukocytosis and anemia. Computed Tomography (CT) abdomen and pelvis showed thickening of the cecum wall and terminal ileum and multiple enlarged mesenteric lymph nodes. Colonoscopy demonstrated ulceration distal to the ileocecal valve, circumferential ulceration and edema of the ileum proximal to the ileocecal valve, severe diverticulosis of the left colon and subcentimeter polyps in the descending colon. Terminal ileum and ascending colon biopsies were consistent with DLBCL, non-germinal center type with CD30 expression. On the day following colonoscopy, the patient developed worsening fevers and abdominal pain, found to have retroperitoneal free air on imaging, concerning for bowel perforation. Immediate surgical consult was obtained and he underwent urgent open right colectomy with diverting loop ileostomy. The presentation of GI-DLBCL is non-specific and subtle, often leading to diagnosis in advanced stages or with serious complications. The literature describes many cases of DLBCL that are resistant to chemotherapy and diagnosis often occurs once disease has progressed too far to tolerate treatment. Despite its increasing incidence, there is currently no large prospective study or evidence-based medical evidence to provide clear guidance on treatment decisions for this specific type of lymphoma. Therefore, early recognition may contribute to improved outcomes and development of better treatment regimens for GI-DLBCL.
Case Description/
Methods:
Discussion: 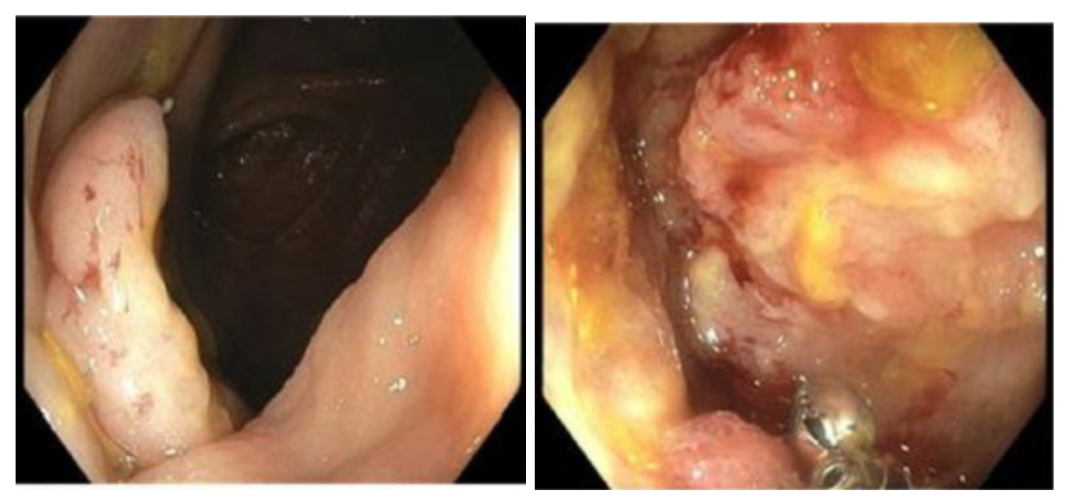
Figure: CT Abdomen and Pelvis images of demonstrating thickening of the cecum wall and terminal ileum and enlarged mesenteric lymph nodes. 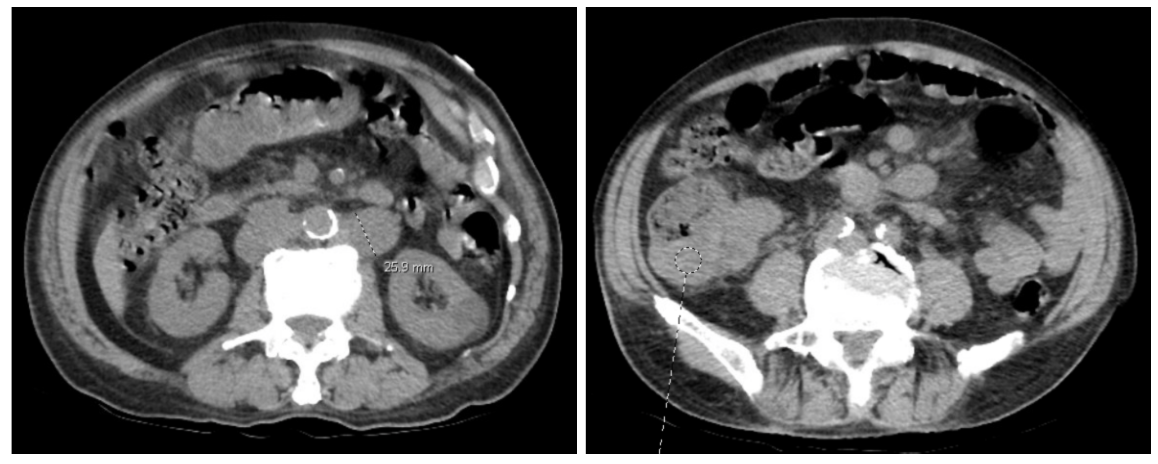
Figure: Endoscopic image of ulcerated lesion just distal to ileocecal valve and circumferential ulceration and edema of the ileum proximal to the ileocecal valve.
Disclosures:
Nupur Savalia indicated no relevant financial relationships.
Sevag Hamamah indicated no relevant financial relationships.
Faizi Hai indicated no relevant financial relationships.
Nupur Savalia, MD, Sevag Hamamah, MD, Faizi Hai, MD. P4608 - Primary Gastrointestinal Diffuse Large B Cell Lymphoma Presenting as Ileocecal Mass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.