Robert Wood Johnson Medical School, Rutgers University New Brunswick, NJ
Naveen Mallangada, MD1, Pooja Jotwani, MD2, Anish V. Patel, MD2 1Robert Wood Johnson Medical School, Rutgers University, Jericho, NY; 2Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ Introduction: Giant Cell Arteritis (GCA) is the most common idiopathic systemic vasculitis in adults over 50 years of age. Common reported symptoms are unintentional weight loss, headache, jaw claudication, fever and visual loss. Gastrointestinal specific presentations of GCA related to large vessel disease are atypical, rare, minimally reported, and variable in presentation.
Case Description/
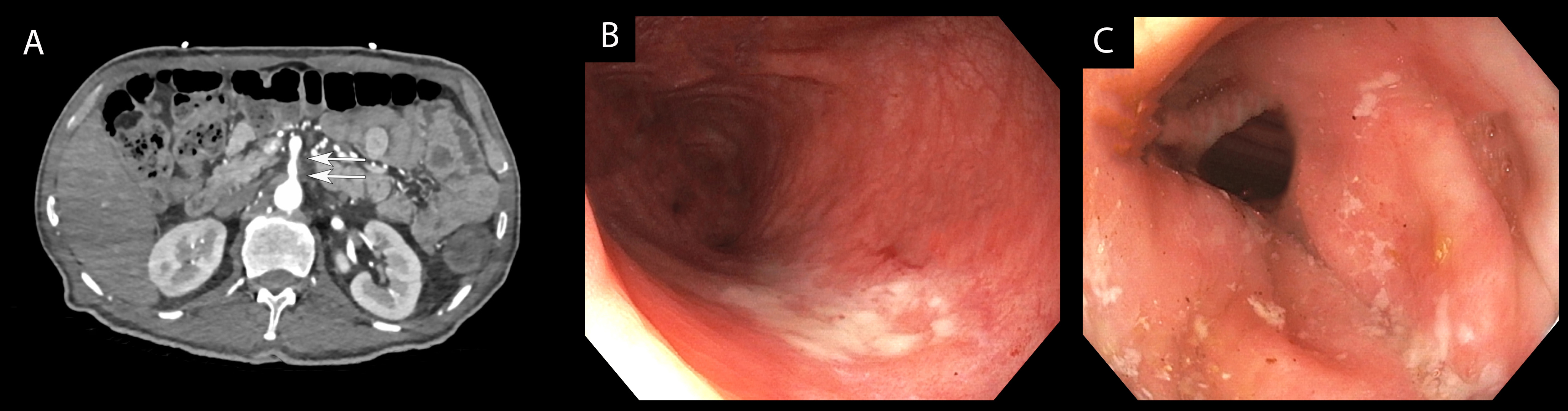
Methods: A 64-year-old Hispanic male with type II diabetes and hypertension presented to the emergency room due to vasovagal syncope during attempted defecation. He reported an unintentional 10 lb weight loss in the setting of one month of progressively worsening constipation and post-prandial lower abdominal pain with associated poor appetite and reduced oral intake. He did also endorse intermittent bitemporal headaches and jaw claudication during this time. His last bowel movement was four days prior to presentation. CT angiogram revealed irregular multifocal enhancement of the abdominal aorta with superior mesenteric artery (Figure 1A) and inferior mesenteric artery involvement, concerning for large vessel arteritis, along with sigmoid colon thickening. ESR and CRP were elevated. Colonoscopy was performed, which found mild inflammation and shallow ulcerations (Figure 1B, C) from the descending colon to the ano-rectal verge. Colon biopsies were supportive of ischemic colitis. Patient underwent temporal artery biopsy given the abnormal CT angiogram findings and clinical symptoms (temporal headache and jaw claudication) with pathology supporting diagnosis of GCA. Patient was discharged with daily bowel regimen, oral steroids, and plan to start tocilizumab as outpatient per rheumatology and vascular surgery teams. His abdominal pain and constipation had resolved at the time of 1-month follow up. Discussion: We report here an atypical presentation of GCA with predominantly GI symptoms of abdominal pain, constipation and weight loss. Mesenteric involvement of GCA is exceptionally rare, with few cases of GCA causing bowel ischemia reported in the literature. A broad differential inclusive of vasculitis should be considered when patients develop new abdominal pain and colonic dysmotility. This case also demonstrates the importance of thorough history taking, review of systems (such as headache and jaw claudication in our patient) and contrast imaging in the evaluation and diagnostic workup of new GI complaints to avoid missing potential systemic disease processes such as vasculitis.
Figure: Image A: CT angiogram detailing irregular multifocal enhancement of the abdominal aorta with superior mesenteric artery involvement; Images B & C: mild inflammation and shallow ulcerations from the descending colon to the ano-rectal verge.
Disclosures: Naveen Mallangada indicated no relevant financial relationships. Pooja Jotwani indicated no relevant financial relationships. Anish Patel indicated no relevant financial relationships.
Naveen Mallangada, MD1, Pooja Jotwani, MD2, Anish V. Patel, MD2. P4727 - A Case of Large Vessel Giant Cell Arteritis Presenting With Abdominal Pain, Constipation, and Unintentional Weight Loss, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")