Asna Aafreen, MD1, Akriti Agrawal, MD1, Solomon Anighoro, MD1, Adishwar Rao, MD2, Hamnah Tayyab, MD1, Asnia Kauser, MD1, Rewanth Katamreddy, MD3, Raja Chandra Chakinala, MD1, John Pamula, MD1 1Guthrie Robert Packer Hospital, Sayre, PA; 2Guthrie Robert Packer Hospital, Department of Internal Medicine, Sayre, PA; 3Guthrie Robert Packer Hospital, Department of Gastroenterology, Sayre, PA Introduction: Colorectal cancer (CRC) is the third leading cause of cancer related death in the United States with increasing mortality rates globally. The aim for QI project was to increase the overall CRC screening rates in Internal Medicine Resident Clinic by 2% from the last PDSA cycle, understanding patient barriers and implementing close follow up.
Methods: Patients were evaluated by residents in clinic. EPIC was utilized for the purpose of identifying a screening gap. Options were discussed with patients in the clinic as well as over the phone. Clinic board tracking was done, patient phone calls were made to obtain consent and initiate scheduling, scheduling issues were addressed. The screening rate was monitored each month for the PDSA cycle. Results: In the PDSA cycle, the Colo-Rectal Cancer Screening rate was increased from 74.5 % to 76.2 %. As of April 2025, CRC screening rates at Robert Packer Hospital, Sayre, Resident Clinic are at goal at 77%. Discussion: Our goal for this project was to increase colorectal cancer screening by 2% during this PDSA cycle; PDSA Cycle 2023-2024 faced their own challenges by addressing scheduling issues between the GI Department and PCPs. By addressing those issues, CRC screening increased by 2%. This PDSA cycle, we were able to increase compliance rates from 74.5 % to 76.2 %. By calling patients and obtaining information about outside hospital compliance, we were able to increase compliance. Additionally, incorporating the information from Cologuard testing helped achieve our goal. This shows an improvement of screening rates with our intervention.
Although, we have shown steady improvement with CRC compliance rates, it remains an area for improvement. Advances in technology and a better understanding of the various environmental and genetic factors at play will give more shape to the screening tools int the future; presently next generation multi-target stool DNA test and cell free DNA blood-based test are among the modalities being studied.
Studies have shown an increase in routine screening by implementing a patient driven decision worksheet and phone follow-up by non-clinical staff.
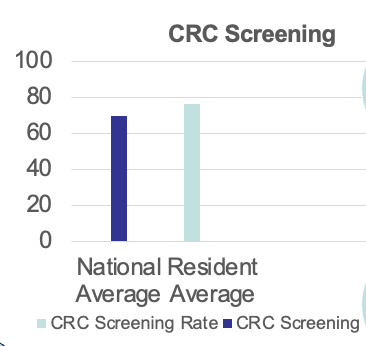
Figure: Comparison of CRC Screening Rates: National Average versus Resident Clinic Average at RPH, Sayre, PA
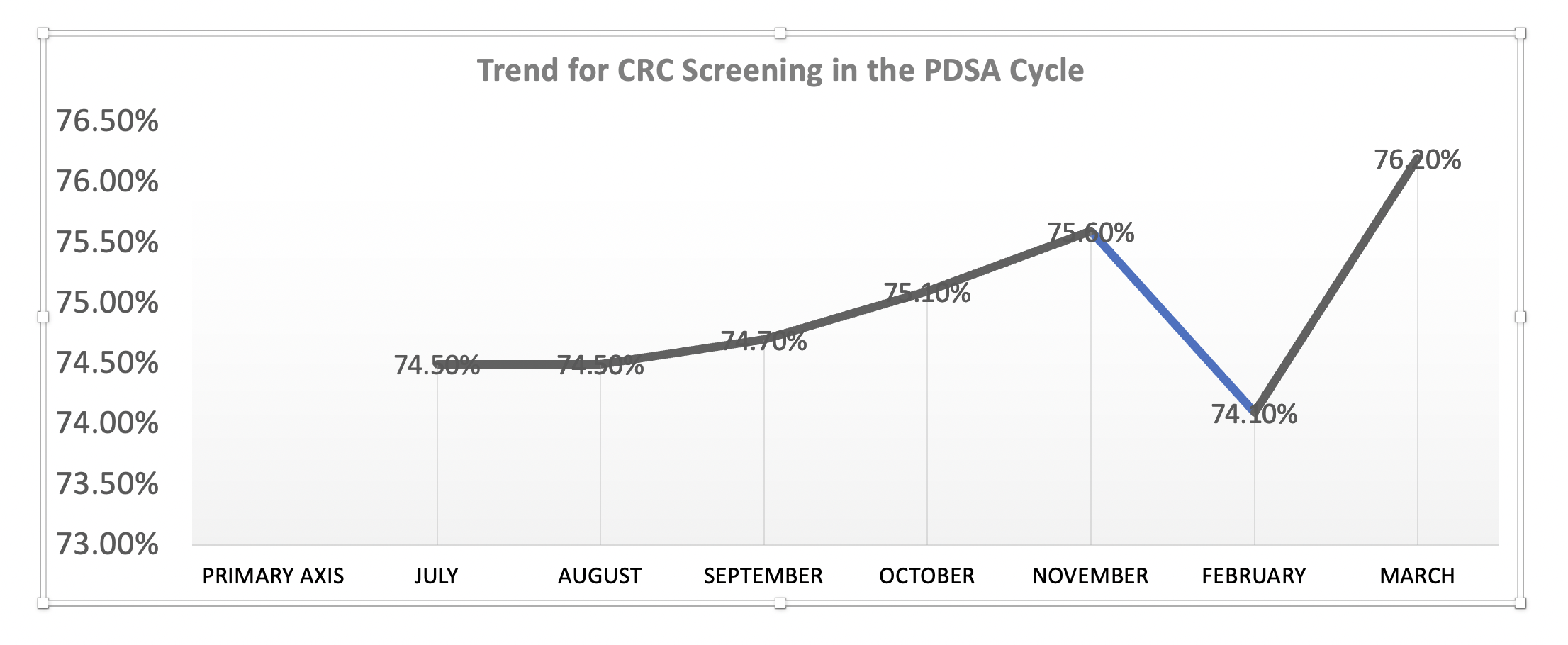
Figure: Trends in CRC Screening PDSA Cycle II 2024-2025 at RPH, Sayre, PA
Disclosures: Asna Aafreen indicated no relevant financial relationships. Akriti Agrawal indicated no relevant financial relationships. Solomon Anighoro indicated no relevant financial relationships. Adishwar Rao indicated no relevant financial relationships. Hamnah Tayyab indicated no relevant financial relationships. Asnia Kauser indicated no relevant financial relationships. Rewanth Katamreddy indicated no relevant financial relationships. Raja Chandra Chakinala indicated no relevant financial relationships. John Pamula indicated no relevant financial relationships.
Asna Aafreen, MD1, Akriti Agrawal, MD1, Solomon Anighoro, MD1, Adishwar Rao, MD2, Hamnah Tayyab, MD1, Asnia Kauser, MD1, Rewanth Katamreddy, MD3, Raja Chandra Chakinala, MD1, John Pamula, MD1. P4796 - Keeping an Eye on the Colon: A QI Approach to Colorectal Cancer Screening in a Resident Internal Medicine Clinic, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.