University of Maryland Medical System Baltimore, CA
Jerry H. Rose, MD1, Nima Sharifai, MD, PhD2, Mohammed Alkahil, MBBS2, Abdulhameed M. Al-Sabban, MBBS3 1University of Maryland Medical System, Baltimore, MD; 2University of Maryland School of Medicine, Baltimore, MD; 3UNIVERSITY OF MARYLAND School of Medicine, Baltimore, MD Introduction: Esophageal nerve sheath tumors are an uncommon type of esophageal submucosal tumors, with fewer than 30 cases reported in the literature.1 They arise from Schwann cells of the peripheral nervous system and are histologically defined by spindle-shaped cells with strong S-100 positivity and a lack of CD117, CD34, smooth muscle actin, and desmin. These tumors typically occur as a solitary lesion in individuals aged 40–70, with a slight female predominance2 and possible links to genetic syndromes such as Neurofibromatosis Type 2 (NF2).3 Due to their rarity, they are often poorly recognized clinically and misdiagnosed before surgery. We present a rare case of esophageal nerve sheath tumor to add to the limited existing data and support a better understanding of this entity.
Case Description/
Methods: A 46-year-old male underwent an upper endoscopy and colonoscopy for work up for iron deficiency anemia. The endoscopy revealed a polypoid submucosal lesion in the esophagus (Paris class Isp) at 37 cm from the incisors. Subsequent EUS revealed a hypoechoic, well-demarcated lesion within the submucosa, measuring 9mm x 7mm x 5mm and 4.6 mm in thickness. The biopsy showed reactive squamous mucosa and subepithelial spindle cell proliferation. Due to concern for malignant potential ESD was performed with complete resection with no complications. Histopathology revealed well-formed subepithelial nodule consisting of localized spindle cell proliferation, Schwann cells, a mixed population of inflammatory cells, and multiple ectatic vessels throughout the lesion. Immunohistochemical analysis was positive for S100, SOX10, Bcl2, along with CD68, CD163, and CD117, indicating a prominent mast cell population and scattered histiocytes. The overall features are suggestive of a benign nerve sheath lesion, with subtypes of neurofibroma and mucosal Schwann cell hamartoma among the differentials. Discussion: This case highlights the importance of including benign nerve sheath lesions in the differential diagnosis of submucosal esophageal masses. Their morphological complexity contributes to diagnostic difficulties and has led to a variety of terms being used historically to describe similar lesions. Submucosal esophageal lesions, while uncommon,1 can be effectively managed with minimally invasive techniques when identified promptly.
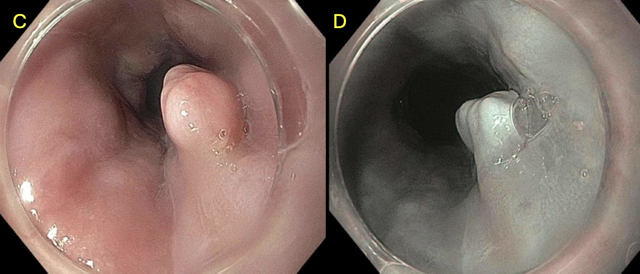
Figure: C. Lower third of esophagus D. Narrow Band Imaging of submucosal mass without pit patterning
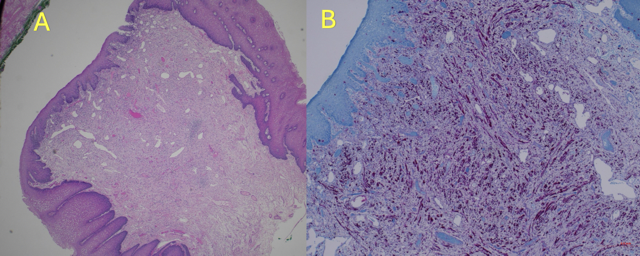
Figure: A. H&E Hematoxylin and eosin. B. Immunostain with S-100 protein positivity, confirming the diagnosis of nerve sheath tumor.
Disclosures: Jerry Rose indicated no relevant financial relationships. Nima Sharifai indicated no relevant financial relationships. Mohammed Alkahil indicated no relevant financial relationships. Abdulhameed Al-Sabban indicated no relevant financial relationships.
Jerry H. Rose, MD1, Nima Sharifai, MD, PhD2, Mohammed Alkahil, MBBS2, Abdulhameed M. Al-Sabban, MBBS3. P4962 - Esophageal Nerve Sheath Tumor: A Rare Benign Tumor With Diagnostic Challenges, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")