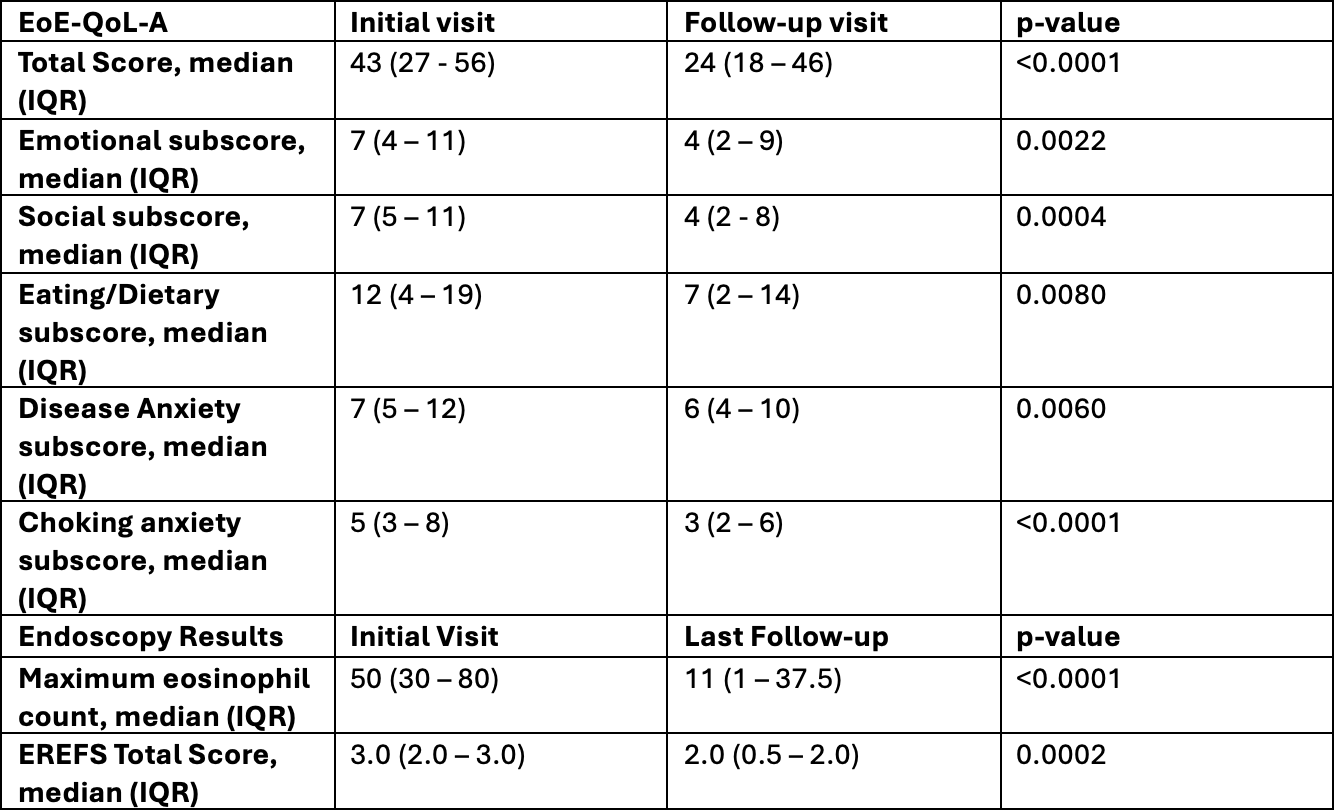
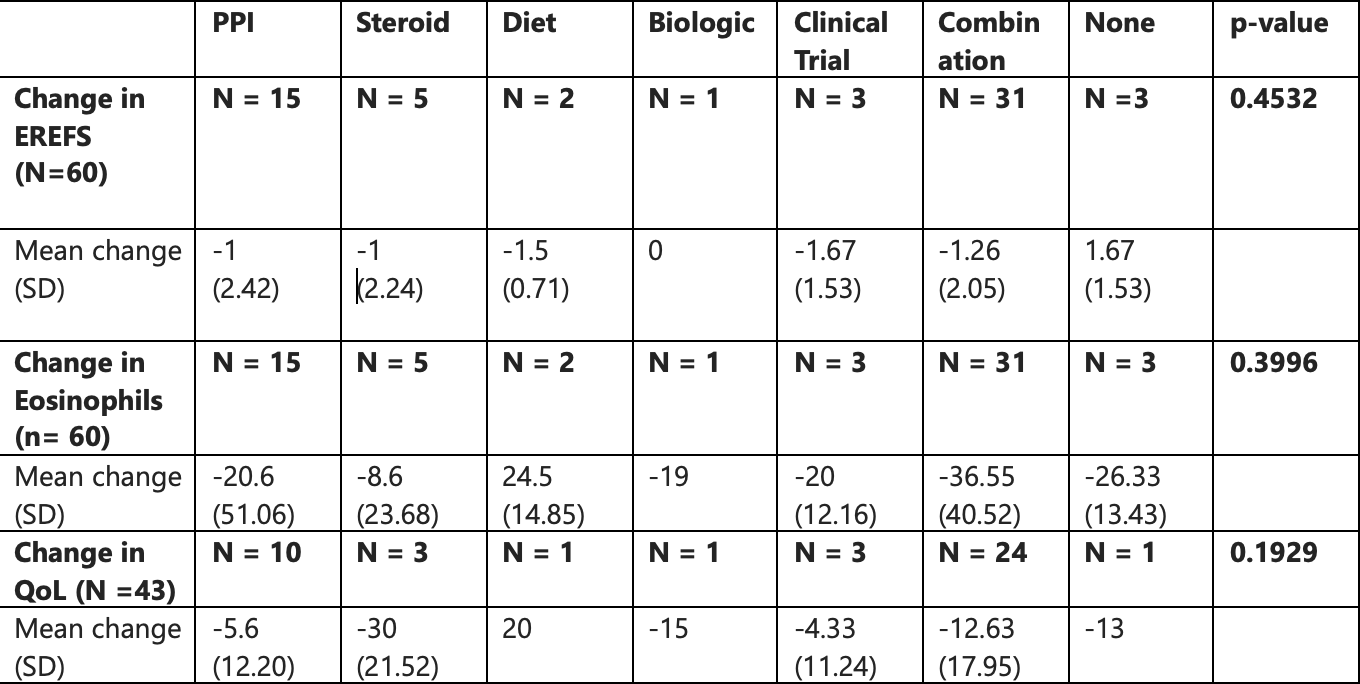
Poshika Dhingra, MD, BSc1, Michaela Quon, 2, Jingru Helen Ha, 2, Igor Stukalin, MD2, Eva Mak, 2, Brooke Maracle, 2, Christopher Ma, MD2, Milli Gupta, MD, BSc2 1University of Alberta, Edmonton, AB, Canada; 2University of Calgary, Calgary, AB, Canada Introduction: Eosinophilic esophagitis (EoE) is a chronic, immune-mediated disease marked by esophageal dysfunction and eosinophil-predominant inflammation in the esophagus. Available treatments include proton pump inhibitors, topical corticosteroids, diet, biologics, and esophageal dilation. However, optimal long-term strategies and their durability remain unclear. EoE also significantly impacts quality of life (QoL) due to dietary restrictions, fear of food impaction, and healthcare utilization. This study explores disease progression, treatment response, and patient-reported outcomes (PROs) in EoE patients from a Canadian clinic. Methods: This prospective cohort study included 60 patients diagnosed with EoE between 2011–2025. Data was collected on demographics, treatments, histology, Eosinophilic Esophagitis Endoscopic Reference Score (EREFS), and Adult Eosinophilic Esophagitis Quality of Life (EoE-QOL-A) questionnaire scores. Wilcoxon signed-rank, Spearman correlation, and ANOVA were used to assess changes from initial consult to follow-up. Results: Among 60 patients (76.7% male, median age 30.4 years [IQR 17.8-36.2]), median disease duration was 6.2 years [IQR 4.4-9.7]. Only 3% did not have a follow-up within 12 months of first assessment. Patients tried an average of 2.28 treatment classes. Eosinophil counts declined from 50 to 11/HPF (p< 0.0001) and EREFS scores improved from 3.0 to 2.0 (p=0.0002) with treatment (Table 1). QoL scores improved from 43 to 24 (p< 0.0001) with treatment, including all subscores (Table 1). History of food bolus impaction did not significantly correlate with poorer QoL (p = 0.1684 at baseline, p = 0.0918 at follow-up). Changes in eosinophil counts and EREFS were not correlated with QoL (ρ = 0.14 and –0.20, p > 0.1). ANOVA showed no significant differences by treatment group for change in eosinophils (p=0.398), EREFS (p=0.99), or QoL scores (p=0.185) (Table 2). Discussion: While significant improvements were seen in eosinophils, EREFS, and QoL over time, no statistical differences were found based on treatment type. This likely reflects small sample size effect. Combination therapies were frequently used in real-world practice prior to the approval of monoclonal antibodies. The lack of correlation between eosinophil counts, EREFS, and QoL demonstrate the complex interplay between objective disease control and patient experiences. The observed improvements in QOL scores with treatment highlight the importance of including PROs in longitudinal care and future trials.
Figure: Table 1: Adult Eosinophilic Esophagitis Quality-Of-Life questionnaire (EOE-QOL-A) scores, maximum eosinophil count/HPF on endoscopic biopsy and median EREFS at initial consult visit and last follow-up visit with treatment between 2003 and 2025. P value <0.05 indicates statistical significance.
Figure: Table 2: Comparison of mean changes in EREFS scores, Eosinophil Counts/HPF on endoscopic biopsies, and QoL Scores by Treatment Type in EoE Patients. P value <0.05 indicates statistical significance.
Poshika Dhingra, MD, BSc1, Michaela Quon, 2, Jingru Helen Ha, 2, Igor Stukalin, MD2, Eva Mak, 2, Brooke Maracle, 2, Christopher Ma, MD2, Milli Gupta, MD, BSc2. P4951 - A Prospective Approach to Disease Progression, Treatment Response and Quality of Life in Eosinophilic Esophagitis From Canada, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")