Matthew Steinberg, MS1, Cynthia Tran, MD2, Steven Keilin, MD2 1Emory University School of Medicine, Atlanta, GA; 2Emory University Hospital, Atlanta, GA Introduction: Choledocholithiasis is a common biliary pathology typically managed via endoscopic retrograde cholangiopancreatography (ERCP). However, anatomic variants or obstructing lesions can complicate biliary access. Duodenal lipomas are rare benign tumors, comprising less than 4% of all gastrointestinal lipomas, and are infrequently found near the ampulla of Vater where they may obscure the major papilla and hinder cannulation [1]. We present a case of successful ERCP and choledocholithiasis extraction following endoscopic resection of an ampulla-obscuring duodenal lipoma.
Case Description/
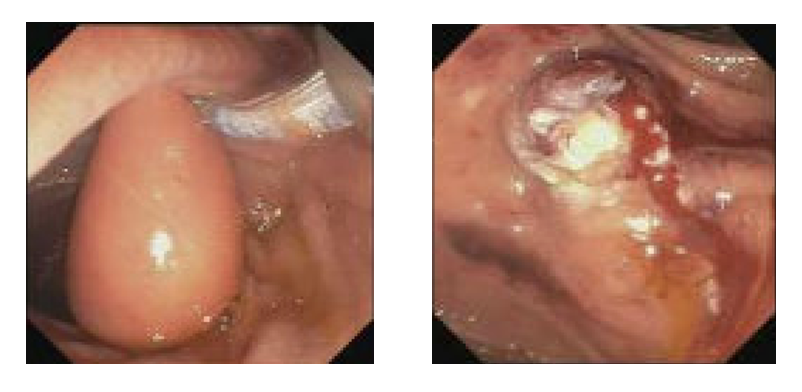
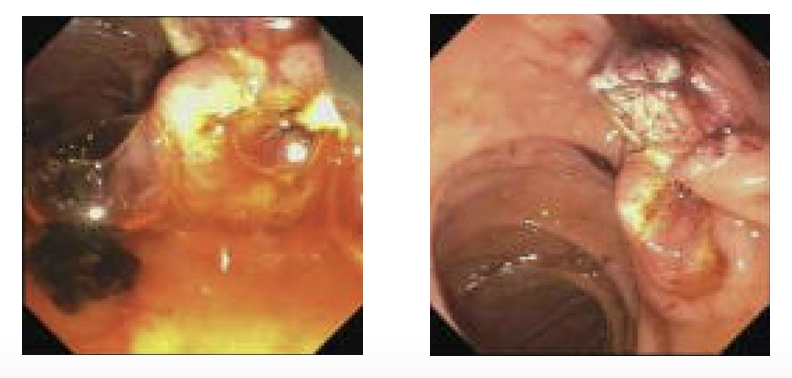
Methods: A 78 y/o male patient undergoing ERCP for choledocholithiasis was found to have a 20 mm pedunculated, polypoid lesion in the second portion of the duodenum overlying the major papilla. The lesion had endoscopic features consistent with a lipoma, including soft consistency and yellowish hue. Multiple attempts to mobilize or reposition the lesion using endoscopic clips failed to improve visualization or cannulation trajectory.
Given the persistent obstruction, a decision was made to resect the lipoma to allow access to the ampulla. The lesion was removed in a piecemeal fashion in two fragments using standard polypectomy techniques. Following resection, the ampulla was visualized, although cannulation remained technically challenging due to a bulging papilla with a long intraduodenal segment.
After successful biliary cannulation, a cholangiogram revealed a filling defect consistent with a single common bile duct stone. Biliary sphincterotomy was performed, and complete stone clearance was achieved using balloon extraction. No stent was placed. The patient received rectal indomethacin and intravenous lactated Ringer’s solution to mitigate the risk of post-ERCP pancreatitis. The patient tolerated the procedure without complications. Discussion: This case highlights a rare cause of ampullary obstruction due to a duodenal lipoma and underscores the importance of recognizing and managing such anatomical barriers during ERCP. While duodenal lipomas are generally asymptomatic, their location can result in diagnostic and therapeutic challenges. Endoscopic resection allowed for definitive management of the underlying choledocholithiasis. This case supports the feasibility and safety of performing endoscopic resection in select scenarios to facilitate biliary access.
[1] Yaman et al. Symptomatic duodenal lipoma with endoscopic snare polypectomy. Ulus Cerrahi Derg. 2014 Jun 1;30(2):103-5.
Figure: Left: Common bile duct stone s/p removal. Right: Duodenum s/p procedure.
Disclosures: Matthew Steinberg indicated no relevant financial relationships. Cynthia Tran indicated no relevant financial relationships. Steven Keilin indicated no relevant financial relationships.
Matthew Steinberg, MS1, Cynthia Tran, MD2, Steven Keilin, MD2. P5749 - Endoscopic Stone Removal After Resection of a Duodenal Lipoma Overlying the Ampulla of Vater, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.