University of Massachusetts Chan Medical School-Baystate Medical Center Springfield, MA
Pranav Ramamurthy, MBBS, MD1, Syed Hamza Sohail, MD2, Tushaar Shrimanker, MD2, Nha Duong, DO3 1University of Massachusetts Chan Medical School-Baystate Medical Center, Springfield, MA; 2University of Massachusetts Chan Medical School - Baystate Health, Springfield, MA; 3University of Massachusetts Chan Medical School-Baystate Medical Center, Granby, CT Introduction: Breast cancer metastasis to the gastrointestinal tract is exceedingly rare with only a handful of reports in the literature. We report a case of common bile duct (CBD) metastasis leading to cholecystitis and biliary obstruction and the invaluable role of endoscopic ultrasound (EUS) in diagnosis and subsequent management.
Case Description/
Methods: An 82-year-old woman recently diagnosed with localized lobular breast carcinoma presented to our institution with several days of upper abdominal pain, nausea, vomiting and chills. Workup revealed a normal bilirubin with mildly elevated transaminases and alkaline phosphatase. Abdominal computed tomography (CT) revealed cholelithiasis, gallbladder (GB) wall thickening consistent with cholecystitis, and dilated intrahepatic ducts. Subsequent magnetic resonance cholangiopancreatography demonstrated a stricture in the CBD (Figure 1). EUS revealed a subtle hypoechoic mass in the mid-CBD region at the area of cystic duct insertion (Figure 2). There was dilatation of the upstream bile duct as well as cystic duct indicative of a malignant obstruction. The mass was sampled with fine needle biopsy, followed by endoscopic retrograde cholangiopancreatography (ERCP) with placement of a plastic stent in the CBD. Pathology was consistent with metastatic lobular breast cancer. The patient remained symptomatic despite plastic stent placement and was not a surgical candidate for cholecystectomy. Repeat ERCP was performed, and the plastic stent was replaced with a metal stent given confirmation of metastatic disease. EUS-guided transmural drainage of the GB was performed for cholecystitis with placement of a lumen apposing metal stent (LAMS). Her symptoms completely resolved after the procedure. Two months later, a repeat endoscopy was performed with clearance of GB stones and subsequent LAMS removal. A double-pigtail stent was placed across the fistula to maintain patency. The patient remained asymptomatic at follow up. Discussion: This is a rare case of breast cancer metastasis to the biliary system causing biliary and cystic duct obstruction with resultant cholecystitis due to the location of the tumor. EUS allowed us to detect and sample the CBD metastasis even before it was visible on cross sectional imaging. This is turn led to appropriate and timely endoscopic interventions with favorable outcomes in an otherwise non-surgical candidate, highlighting the importance of EUS in management of complex malignant biliary disease.
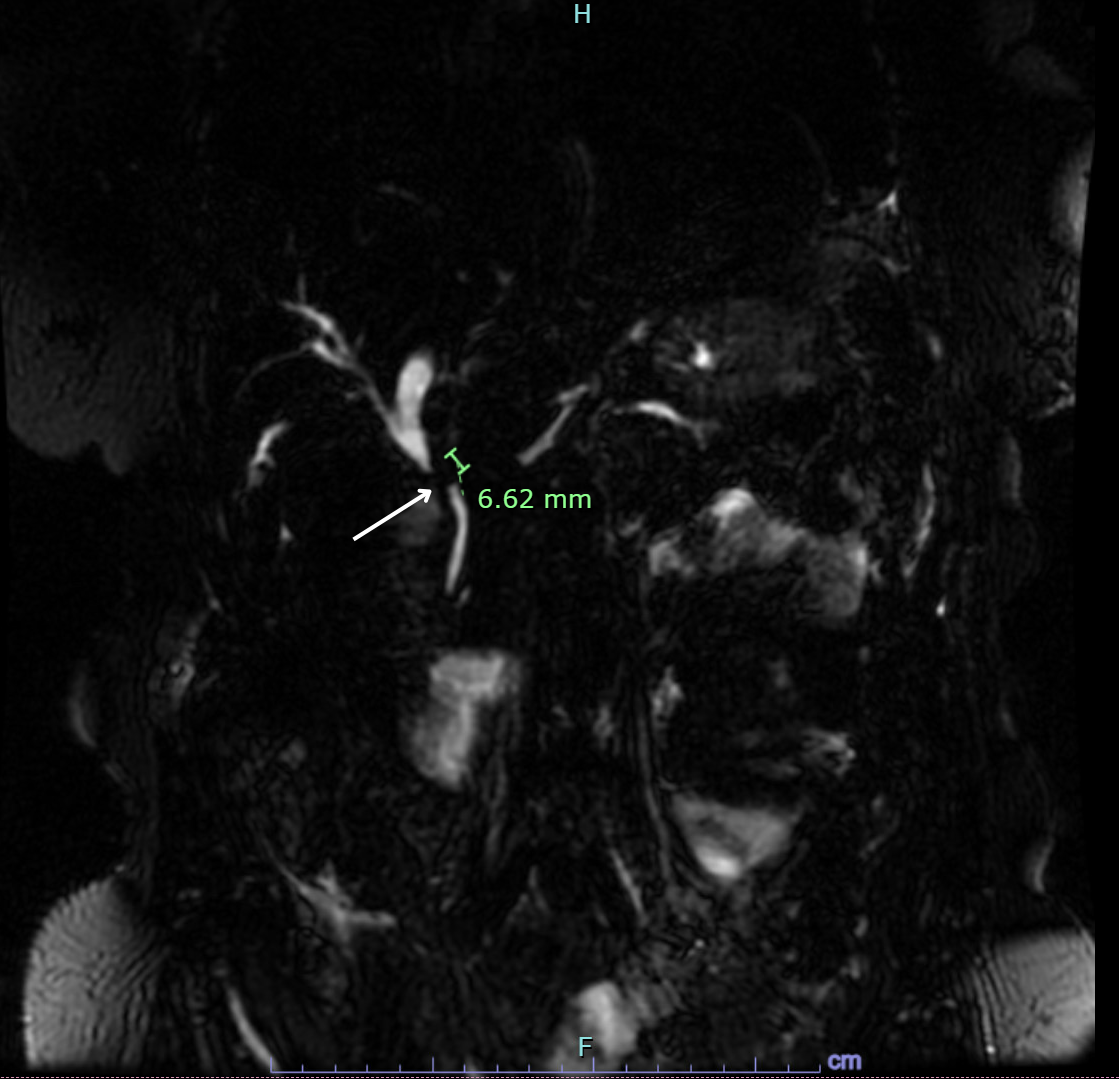
Figure: Figure 1: Magnetic resonance cholangiopancreatography showing moderate intrahepatic biliary ductal dilatation with abrupt cut off at the proximal common hepatic duct demonstrating a 6.6mm stricture (white arrow). No obvious mass noted on imaging.
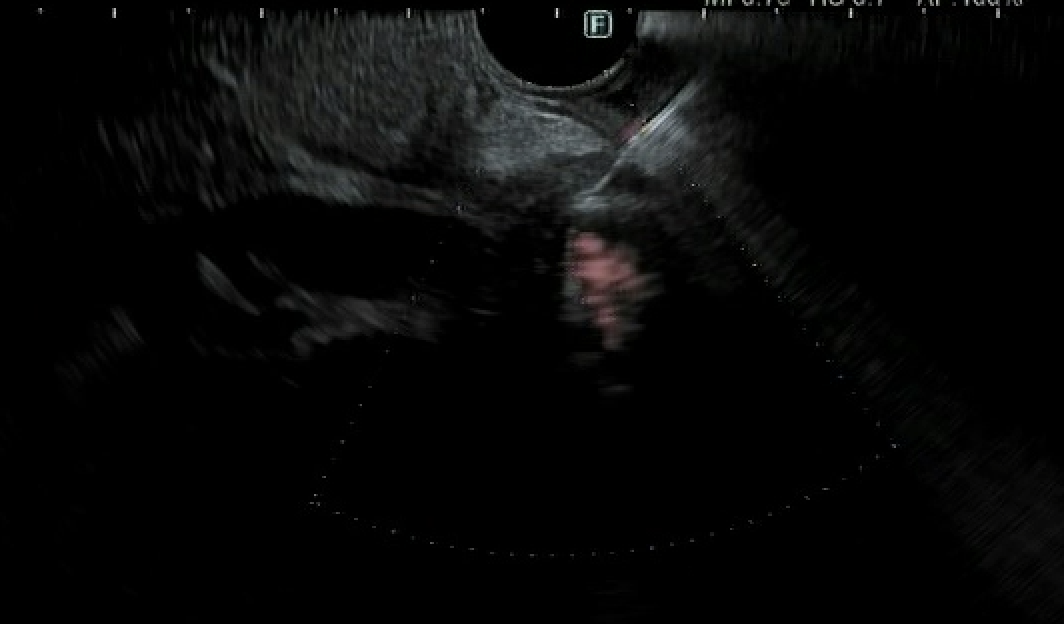
Figure: Figure 2: Endoscopic ultrasound imaging demonstrating a subtle hypoechoic mass in the mid-CBD region at the area of cystic duct insertion being sampled with fine needle biopsy.
Disclosures: Pranav Ramamurthy indicated no relevant financial relationships. Syed Hamza Sohail indicated no relevant financial relationships. Tushaar Shrimanker indicated no relevant financial relationships. Nha Duong indicated no relevant financial relationships.
Pranav Ramamurthy, MBBS, MD1, Syed Hamza Sohail, MD2, Tushaar Shrimanker, MD2, Nha Duong, DO3. P5745 - Invaluable Role of Endoscopic Ultrasound in a Rare Case of Metastatic Breast Cancer to the Bile Duct, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Pranav Ramamurthy, MBBS, MD (he/him/his) photo")