University of North Carolina at Chapel Hill Chapel Hill, NC
Bhagyashree Behera, BS1, Todd H.. Baron, MD1, Alfred Barritt, MD, MSCR, FACG2, Andrew Canakis, DO2 1University of North Carolina at Chapel Hill, Chapel Hill, NC; 2University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC Introduction: While gallstones are common in the American population, gallstone ileus is now a rare complication due to the widespread use of cholecystectomy as well as endoscopic interventions for choledocholithiasis. We present a novel case of gallstone ileus years after cholecystoduodenostomy with an AXIOS stent.
Case Description/
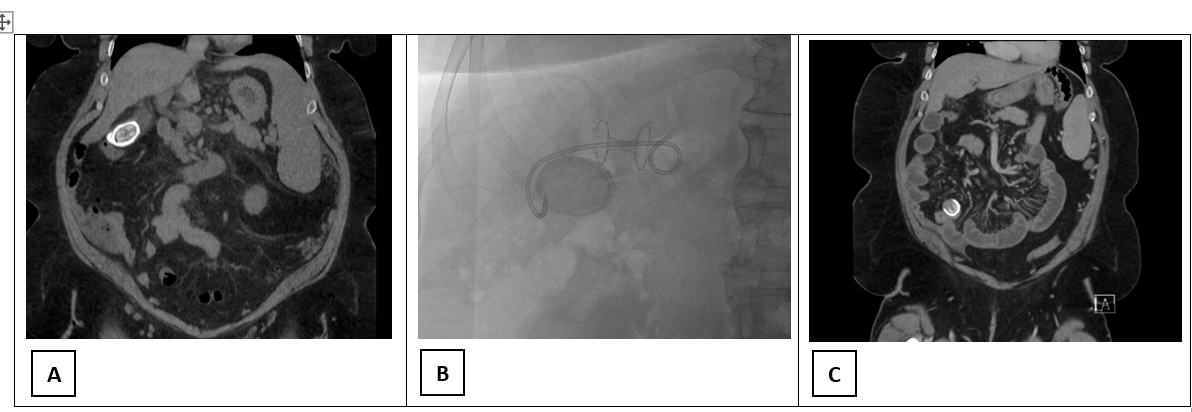
Methods: 46-year-old woman with a past medical history of metabolic-associated steatohepatitis (MASH) cirrhosis, complicated by portal hypertension with Grade I esophageal varices, portal vein thrombosis, splenomegaly, and thrombocytopenia presented to the emergency department with biliary colic. CT imaging revealed a prominent 3.2 cm gallstone [Figure 1A], however, due to the patient’s complicated medical history, body mass index >40kg/m2, and intra-abdominal varices, the patient was determined to be an unsuitable candidate for laparoscopic cholecystectomy. The patient was treated symptomatically for biliary colic and discharged.
After a year of continued biliary colic symptoms, the patient underwent an EUS-guided cholecystoduodenostmy using a lumen-apposing metal stent (LAMS (AXIOS-EC, Boston Scientific, Marlborough, MA) with an indwelling plastic double pigtail biliary stent [Figure 1B]. The stent decompressed the gall bladder and relieved the patients’ symptoms of biliary colic.
Three years later, the patient presented with right lower quadrant pain, nausea and vomiting. The patient’s CT scan and symptoms were consistent with small bowel obstruction from gallstone ileus [Figure 1C] and a cholecystoduodenal fistula. The 3 cm gallstone was trapped in the terminal ileum and unable to pass through the ileocecal valve. The patient successfully underwent an emergency exploratory laparotomy and stone was extracted successfully with clinical resolution. Discussion: Gallstone ileus is an extremely rare complication of large gallstones and occurs due to the formation of a cholecystoduodenal fistula. The fistula is usually a result of chronic inflammation of the gallbladder wall which forms abnormal adhesions to nearby tissue, such as on the duodenum. In this case, the fistula was formed artificially through the placement of LAMS, which created an open channel between the gallbladder and duodenum. Providers could consider destruction of such large stones to avoid future obstruction.
Figure: Figure 1: A: CT scan demonstrating large gallstone in gallbladder. B: Fluoroscopy showing AXIOS stent with pigtail stent. C: Gallstone ileus. Large gallstone impacted in the ileocecal valve with upstream small bowel obstruction
Disclosures: Bhagyashree Behera indicated no relevant financial relationships. Todd Baron: Boston Scientific – Consultant. Cook Endoscopy – Consultant. Olympus America – Consultant. W.L. Gore – Consultant. Alfred Barritt: Boehringer Ingleheim – Consultant. Madrigal – Consultant. Merck – Consultant. Target RWE – Consultant. Andrew Canakis indicated no relevant financial relationships.
Bhagyashree Behera, BS1, Todd H.. Baron, MD1, Alfred Barritt, MD, MSCR, FACG2, Andrew Canakis, DO2. P5742 - Gallstone Ileus: An Unusual Complication Following Transmural Endoscopic Ultrasound-Guided Gallbladder Drainage, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")