Steve Huy D. Phan, BS1, Ashley Huynh, BS2, Aneesa Chowdhury, MD3, John G. Lee, MD3 1UCI School of Medicine, Westminster, CA; 2UC Irvine Digestive Health Institute, Huntington Beach, CA; 3UC Irvine Digestive Health Institute, Orange, CA Introduction: Bouveret syndrome is a rare condition where a large gallstone passes through a bilioduodenal fistula, causing gastroduodenal obstruction. Current literature recommends endoscopic extraction and/or lithotripsy before surgery. However, successful endoscopic management diminishes as gallstones reach greater than 4cm (9.8% vs 66.1%). We present a case where electrohydraulic lithotripsy (EHL) successfully resolves Bouveret syndrome caused by a large gallstone.
Case Description/
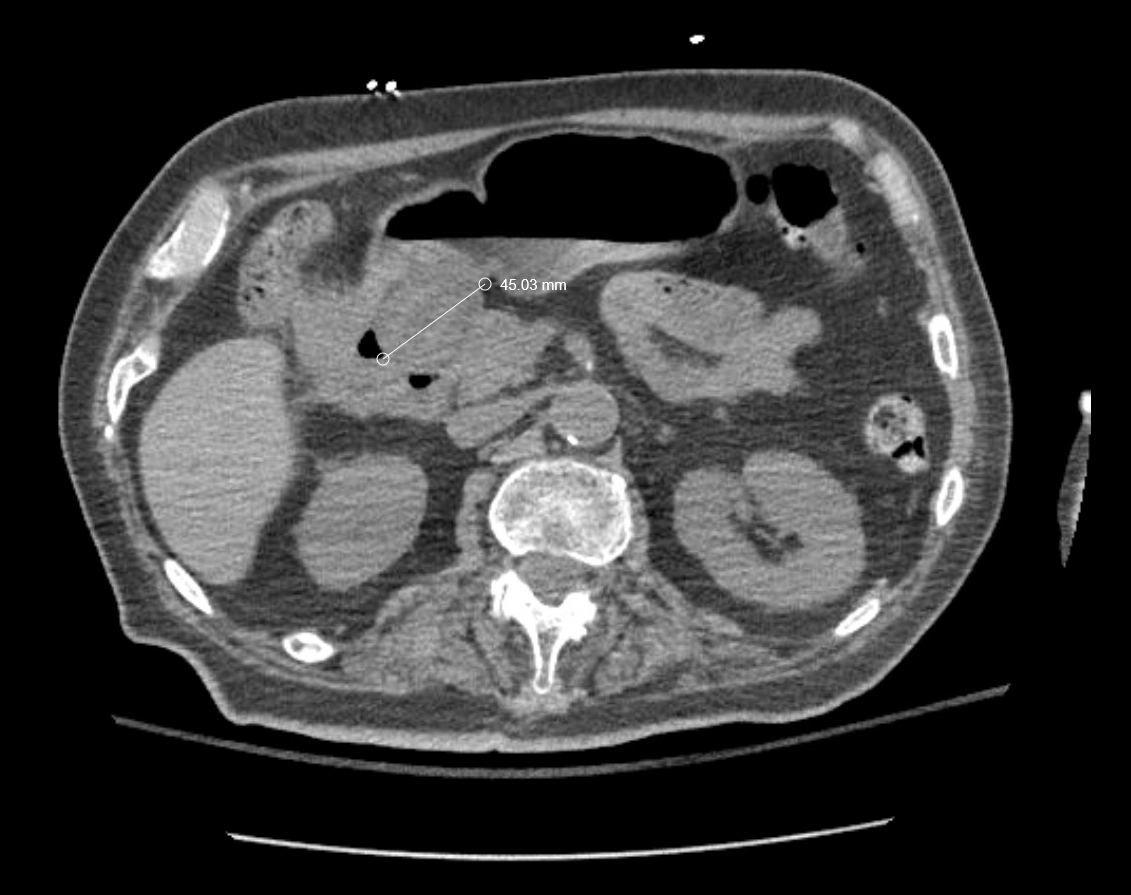
Methods: A 75-year-old man with history of hypertension and diabetes presented to an outside hospital (OSH) with coffee ground emesis for 1 day. Computed Tomography (CT) of the abdomen and pelvis showed 4.5cm lobulated mass eroding into the duodenum and thick-walled gallbladder with extraluminal gas. Initial esophagogastroduodenoscopy (EGD) at OSH found a Mallory-Weiss tear that was clipped and a cholecystoduodenal fistula with a large impacted stone in the proximal duodenum. Following initial stabilization, the patient was referred to our facility for further management.
At our center, EGD confirmed the presence of the impacted gallstone. EHL was then performed to fragment the stone, followed by retrieval of fragments larger than 1cm using lithotripsy baskets and retrieval net. The post-procedure course was uncomplicated, and the patient was subsequently referred to general surgery for an elective laparoscopic cholecystectomy. Discussion: Bouveret syndrome accounts for a small percentage of gallstone ileus cases and poses significant treatment challenges, especially when large gallstones are involved. Endoscopic approaches, while less invasive, have variable success rates, particularly with stones larger than 4 cm. Complications of endoscopic lithotripsy include distal small bowel obstruction due to fragment migration, duodenal perforation, and mucosal injury. However, careful fragmentation and retrieval of sizable stone pieces can mitigate these risks. Our case demonstrates that, with appropriate technique and equipment, endoscopic management can be a viable option even for large gallstones, mitigating the need for more invasive surgical interventions.
Figure: Image 1. Lobulated gallstone seen eroding into proximal duodenum on CT abdomen and pelvis.
Figure: Images 2a. EGD showing large gallstone. 2b. Removal of gallstones using lithotripsy basket.
Disclosures: Steve Huy Phan indicated no relevant financial relationships. Ashley Huynh indicated no relevant financial relationships. Aneesa Chowdhury indicated no relevant financial relationships. John Lee indicated no relevant financial relationships.
Steve Huy D. Phan, BS1, Ashley Huynh, BS2, Aneesa Chowdhury, MD3, John G. Lee, MD3. P5739 - Cracking the Code: Successful Electrohydraulic Lithotripsy of Bouveret Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")