Navi Randhawa, DO1, Deepti Dronamraju, MD2, Sajid Jalil, MD2 1Augusta University, Augusta, GA; 2Stanford University, Palo Alto, CA Introduction: Coccidioidomycosis, caused by Coccidioides immitis, typically manifests as a pulmonary infection in endemic regions such as the southwestern United States. Disseminated coccidioidomycosis (DC) occurs in less than 1% of cases and most commonly affects the skin, bones, or central nervous system. We present a rare case of coccidioidomycosis disseminated to the peritoneum in an immunocompetent male.
Case Description/
Methods: A 51-year-old man with a history of poorly controlled type 2 diabetes mellitus (A1c 10.5), hypertension, and hyperlipidemia presented with progressive abdominal distention, dyspnea and 60-pounds weight loss. A CT scan of abdomen/pelvis revealed mild liver nodularity, moderate ascites with infiltration of omentum. CT chest demonstrated a right lower lobe cavitary lung lesion. He was hospitalized for ascites and work up for malignancy.
On admission, labs on admission platelets of 726, AST of 36, ALT of 27, T bili o 0.3, alk phos of 230, INR of 1.2. He underwent two large-volume paracenteses (7.2 L and 7 L). Fluid analysis revealed high protein (5.8 g/dL) and low SAAG (< 1.1). Fluid cytology was negative for malignancy. Hepatitis serologies were negative. The diagnosis was clinched when fungal culture of the peritoneal fluid came back positive for Coccidioides immitis. The patient was started on fluconazole 400 mg daily. The patient improved clinically without recurrence of ascites accumulation. Repeat CT scan 3 months later, showed improving infiltrate in the right lung base and omentum with complete resolution of ascites. The plan is to continue fluconazole long term and monitor with repeat CT in three months. Discussion: This case illustrates a rare presentation of DC with peritoneal involvement masquerading as malignancy and suspected cirrhosis. Peritoneal involvement of DC is exceedingly rare, especially in immunocompetent patients. High-protein, low-SAAG ascites should prompt consideration of infectious or malignant etiologies, especially when liver function is preserved. In endemic regions, Coccidioides should remain on the differential for unexplained ascites, particularly in immunocompromised hosts such as those with poorly controlled diabetes. Early recognition and initiation of antifungal therapy can prevent unnecessary interventions and improve outcomes. This case adds to the limited literature on coccidioidal peritonitis and highlights the need for increased clinical awareness of its diverse manifestations.
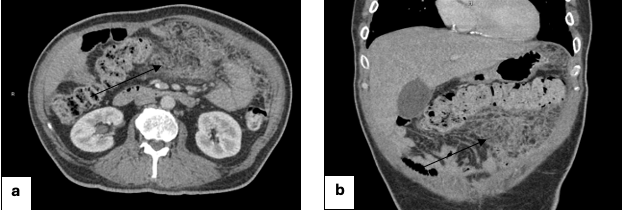
Figure: Figures 1a-b. Outside CT images showing extensive ascites and inflammation/infiltration of omentum.
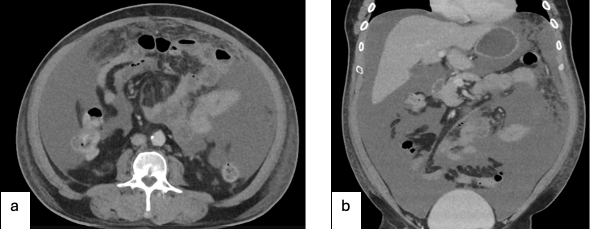
Figure: Figures 2a-b. Extensive peritoneal and omental stranding 2 months later and marked improvement in ascites on long term anti-fungal therapy with oral fluconazole.
Disclosures: Navi Randhawa indicated no relevant financial relationships. Deepti Dronamraju indicated no relevant financial relationships. Sajid Jalil indicated no relevant financial relationships.
Navi Randhawa, DO1, Deepti Dronamraju, MD2, Sajid Jalil, MD2. P5965 - Beyond the Lungs: A Rare Case of Ascites Due to Peritoneal Involvement in Disseminated Coccidioidomycosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.