North Shore University Hospital - Northwell Health Manhasset, NY
Jade Pace, MD1, Ahmed Aboseria, MD2, Justin Lin, MD3, Michael Attanasi, MD4, Anwesha Satapathy, BS1, William Han, BS1, Bheesham Dayal, MD, MPH, CCRP1, Sanjaya Satapathy, MD1 1North Shore University Hospital - Northwell Health, Manhasset, NY; 2North Shore University Hospital - Northwell Health, Brooklyn, NY; 3Northwell Health, New Hyde Park, NY; 4Northwell Health, Manhasset, NY Introduction: Early extubation after liver transplantation (OLT) improves outcomes, but optimal timing remains unclear. The El Moheb Fast-Track Score (FTScore) was proposed to predict early extubation post-OLT. This study aimed to externally validate this score and to identify factors, including frailty, associated with time to extubation. Methods: Adult OLT recipients at our institution from December 2019 to November 2024 were prospectively enrolled (n=288). For FTScore validation, scores were calculated (MELD score < 29 [1 point], packed red blood cells [pRBC] < 4 units [2 points], fresh frozen plasma [FFP] < 4 units [1 point]; max 4 points), and the association with extubation within 4 hours and overall time to extubation was assessed. Preoperative data including Liver Frailty Index (LFI), Karnofsky Performance Scale (KPS), eGFR, and intraoperative factors such as blood product utilization were collected. Statistical analyses included Student’s t-test, bivariate correlation, Kaplan-Meier analysis, and Cox proportional hazard modeling to identify predictors of time to extubation. Results: Eighteen patients (6%) were extubated within 4 hours. They required less intraoperative pRBC (5.17 ± 3.43 vs 10.93 ± 9.02, p < 0.001), FFP (2.94 ± 3.12 vs 8.71 ± 8.32, p < 0.001), and total blood products (11.39 ± 9.24 vs 26.37 ± 21.24, p < 0.001). However, the FTScore was not associated with extubation within 4 hours nor with overall time to extubation.
Shorter time to extubation correlated with higher KPS (r = -0.286, p < 0.001), lower LFI (r = 0.184, p = 0.006), higher pre-transplant eGFR (r = -0.166, p = 0.006), male sex (16.8 ± 18.2 hours vs 23.1 ± 26.9 hours for females, p = 0.034), and lower total blood products (r = 0.262, p < 0.001). MELD 3.0 score, pre-transplant length of stay, race, and malnutrition were not significantly correlated with extubation time.
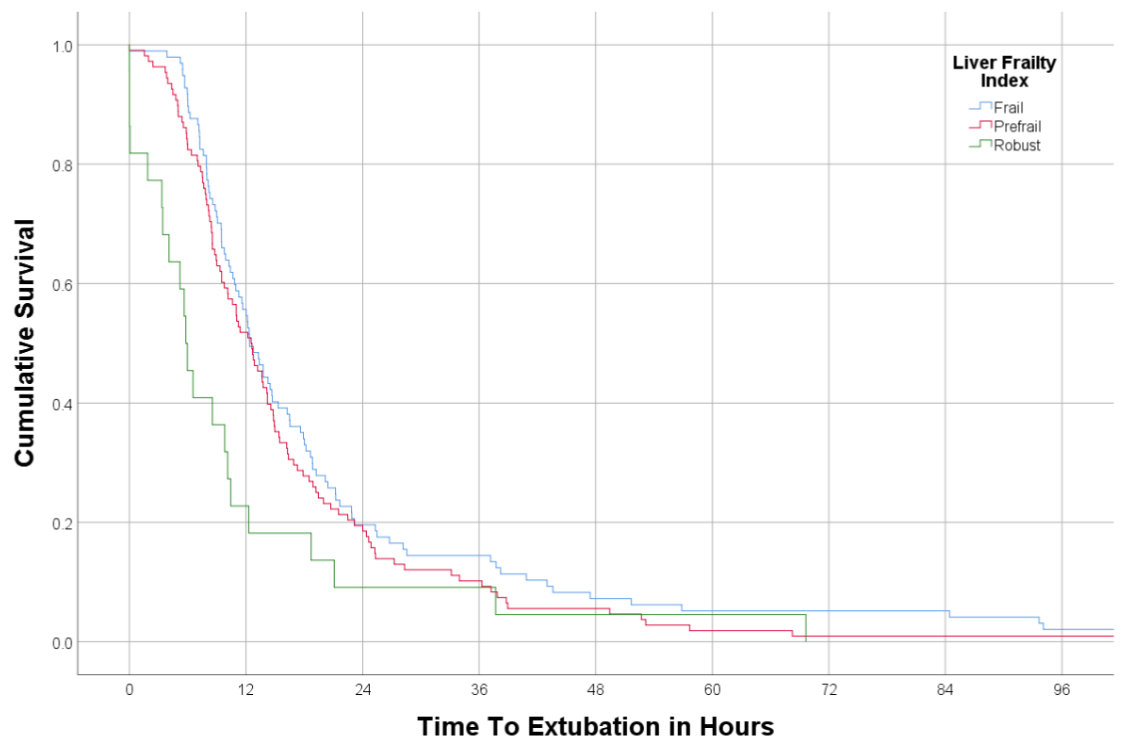
Adjusting for sex, KPS, LFI, and eGFR, only LFI was an independent predictor of time to extubation (HR = 0.799 per unit LFI, 95% CI [0.685 - 0.931], p = 0.004). There was a significant difference in time to extubation across LFI categories (robust, pre-frail, frail; Log Rank p = 0.011, Figure 1). Discussion: The FTScore was not validated in our OLT cohort. However, our analysis identified LFI as a significant independent predictor of extubation time, with frailty being strongly associated with prolonged intubation. While scoring systems like the FTScore have benefits, LFI appears to be a more robust indicator for predicting post-OLT recovery milestones.
Figure: Figure 1: Kaplan-Meier survival curve for Liver Frailty Index vs extubation time.
Disclosures: Jade Pace indicated no relevant financial relationships. Ahmed Aboseria indicated no relevant financial relationships. Justin Lin indicated no relevant financial relationships. Michael Attanasi indicated no relevant financial relationships. Anwesha Satapathy indicated no relevant financial relationships. William Han indicated no relevant financial relationships. Bheesham Dayal indicated no relevant financial relationships. Sanjaya Satapathy indicated no relevant financial relationships.
Jade Pace, MD1, Ahmed Aboseria, MD2, Justin Lin, MD3, Michael Attanasi, MD4, Anwesha Satapathy, BS1, William Han, BS1, Bheesham Dayal, MD, MPH, CCRP1, Sanjaya Satapathy, MD1. P5906 - External Validation of a Fast-Track Extubation Score and Predictors of Extubation Time Following Liver Transplantation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")