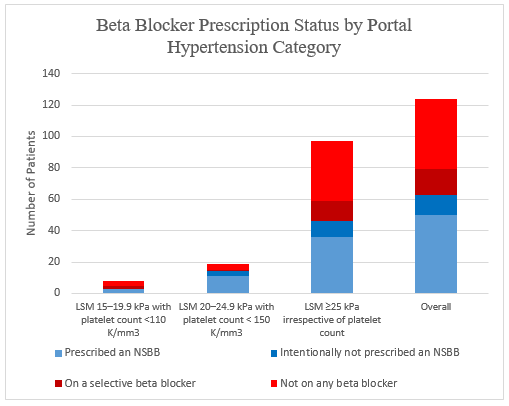
Jesse Silverman, MD1, Aaron Schluger, MD1, Yosef Tobi, BS2, Maxwell Charlat, MD1, Edward Lebovics, MD1 1Westchester Medical Center, Valhalla, NY; 2New York Medical College, Valhalla, NY Introduction: Portal hypertension is a major complication of cirrhosis, increasing the risk of variceal bleeding, ascites, and encephalopathy. Noninvasive markers such as liver stiffness measurement (LSM) and platelet count are now used to guide non-selective beta blocker (NSBB) therapy, as outlined by AASLD criteria and Baveno VII consensus. We aimed to assess adherence to these criteria at our institution and identify opportunities to improve NSBB prescribing. Methods: We retrospectively reviewed all Fibroscan results from January 1st, 2024 to May 14th, 2025, and identified patients with LSM ≥ 15 kPa. Platelet counts within three months before or after the Fibroscan were collected. Patients were grouped according to guideline-based NSBB indication: LSM 15–19.9 kPa with platelet count < 110 K/mm3 (group 1), LSM 20–24.9 kPa with platelet count < 150 K/mm3 (group 2), and LSM ≥ 25 kPa irrespective of platelet count (group 3). NSBB prescription status and reasons for non-prescription were recorded. Results: Among 124 patients who met noninvasive criteria for NSBB, 50 (40%) were prescribed an NSBB, 13 (10%) were intentionally not prescribed an NSBB due to intolerance or status post-TIPS, 16 (13%) were on a selective beta blocker, and 45 (36%) were not on any beta blocker. Combining NSBB prescriptions and intentional non-prescriptions, 63 patients (51%) were managed with guideline-concordant care. When stratified by group, group 1 (n=8) had 38% guideline-concordant care (3 on an NSBB), group 2 (n=19) had 74% guideline-concordant care (11 on an NSBB, 3 intentionally not on an NSBB), and group 3 (n=97) had 47% guideline-concordant care (36 on an NSBB, 10 intentionally not on an NSBB) (Figure 1). Lack of documentation, awaiting EGD or repeat Fibroscan, and missed or no scheduled follow-up accounted for cases of non-adherence to guidelines. Discussion: Adherence to NSBB initiation can be improved at our institution, with many eligible patients not prescribed NSBB without documented rationale. Outdated reliance on further invasive testing and missed or no scheduled follow-up contribute to non-adherence. Improved provider education and systematic prompts may enhance guideline-based NSBB prescribing and preventive care in portal hypertension.
Figure: Beta Blocker Prescription Status by Portal Hypertension Category
Disclosures: Jesse Silverman indicated no relevant financial relationships. Aaron Schluger indicated no relevant financial relationships. Yosef Tobi indicated no relevant financial relationships. Maxwell Charlat indicated no relevant financial relationships. Edward Lebovics indicated no relevant financial relationships.
Jesse Silverman, MD1, Aaron Schluger, MD1, Yosef Tobi, BS2, Maxwell Charlat, MD1, Edward Lebovics, MD1. P5903 - Noninvasive Assessment of Portal Hypertension and Provider Initiation of Non-Selective Beta-Blocker Therapy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Jesse Silverman, MD photo")