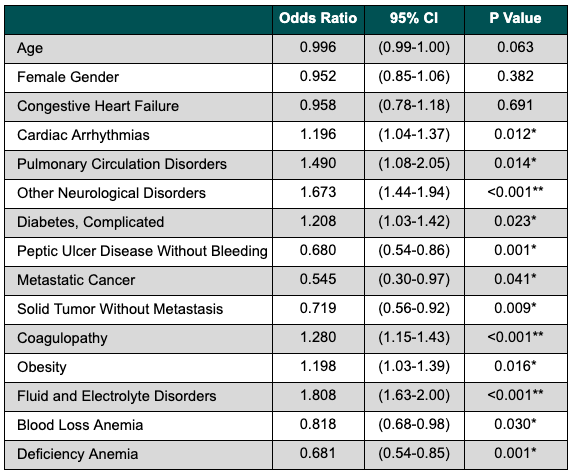
Aya Akhras, MD1, Waseem Wahood, MD, MS2, Azizullah Beran, MD3, Bisher Sawaf, MD4, Asad Ur Rahman, MD5 1HCA Florida Aventura Hospital, Aventura, FL; 2University of Miami Miller School of Medicine, Miami, FL; 3Indiana University School of Medicine, Indianapolis, IN; 4The University of Toledo, Toledo, OH; 5Cleveland Clinic Florida, Weston, FL Introduction: Pre-emptive TIPS (transjugular intrahepatic portosystemic shunt) in high-risk patients with cirrhosis and variceal bleeding has been described as a proactive approach to improve survival and reduce re-bleeding compared to standard medical and endoscopic therapy. This study compares outcomes of pre-emptive TIPS versus therapeutic endoscopy (EGD) in high-risk patients with decompensated cirrhosis and acute variceal bleeding. Methods: We utilized the Nationwide Readmissions Database (NRD), from 2010-2019. We included high risk patients with cirrhosis (Child-Pugh C 10–13 or Child-Pugh B with active bleeding) who were admitted for variceal upper GI bleeds and received endoscopic intervention. The patients were divided into 2 groups: therapeutic EGD + pre-emptive TIPS (within 72 hours of index bleed) versus therapeutic EGD (variceal band ligation) alone. Primary endpoints include 30 and 90-day unplanned readmissions. Secondary endpoints include readmissions for GI bleed, intracranial hemorrhage (ICH) or blood transfusions. Multivariable hierarchical regression was performed, adjusted for age, sex and comorbidities. Data was analyzed using STATA software. P value of < 0.05 was considered significant. Results: A total of 112,674 patients were identified; of these, 4,922 (4.4%) underwent pre-emptive TIPS. Patients in the TIPS group were sicker at baseline (Elixhauser Scaled Score 34.3 (13.4) vs 31.2 (13.3); p< 0.001). Predictors of receiving TIPS are detailed in Table 1. The TIPS group had a higher odds of unplanned 30-day (OR 1.37; p< 0.001) and 90-day readmissions (OR 1.15; p=0.04) compared to patients who received therapeutic EGD only. However, the TIPS group had lower 30-day (OR 0.34; p< 0.001) and 90-day (OR 0.32; p< 0.001) odds of readmission for GI bleed. The TIPS group had lower odds of blood transfusion at both 30 days (OR 0.64; p=0.003) and 90 days (OR 0.59; p< 0.001). There was no significant difference in 30-day or 90-day readmissions for ICH (30-day OR 0.63, p=0.67; 90-day OR 1.15, p=0.86) between groups. Discussion: Therapeutic EGD combined with pre-emptive TIPS in high-risk patients with decompensated cirrhosis and variceal bleeding was associated with reduced readmissions for GI bleeding and lower blood transfusion requirements. However, it was linked to higher overall unplanned readmission rates. Further studies incorporating additional factors like hepatic encephalopathy are needed to fully understand these associations.
Figure: Table 1. Predictors of Receiving Pre-emptive TIPS Among High-Risk Patients with Cirrhosis and Variceal Upper GI Bleed
Disclosures: Aya Akhras indicated no relevant financial relationships. Waseem Wahood indicated no relevant financial relationships. Azizullah Beran indicated no relevant financial relationships. Bisher Sawaf indicated no relevant financial relationships. Asad Ur Rahman: Abbvie Inc – Speakers Bureau.
Aya Akhras, MD1, Waseem Wahood, MD, MS2, Azizullah Beran, MD3, Bisher Sawaf, MD4, Asad Ur Rahman, MD5. P5834 - National Outcomes of Preemptive TIPS in High-Risk Patients with Cirrhosis and Variceal Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.