Ashwariya Ohri, MBBS1, Preeyati Chopra, MBBS2, Mayank Goyal, MBBS3, Dave Buttar, MBBS3, Manik Aggarwal, MD3, Nayantara Coelho-Prabhu, MBBS, FACG3 1Mayo Clinic, Indianapolis, IN; 2Mayo Clinic, Hartford, CT; 3Mayo Clinic, Rochester, MN Introduction: Major bleeding following percutaneous endoscopic gastrostomy (PEG) tube placement is rare, with reported incidence of arterial hemorrhage ranging from 0% to 2.5%. While retroperitoneal bleeding and minor oozing are documented, isolated transection of the gastroepiploic artery causing intraperitoneal hemorrhage requiring laparotomy remains unreported. This case highlights a life-threatening complication in a high-risk patient after a PEG placement.
Case Description/
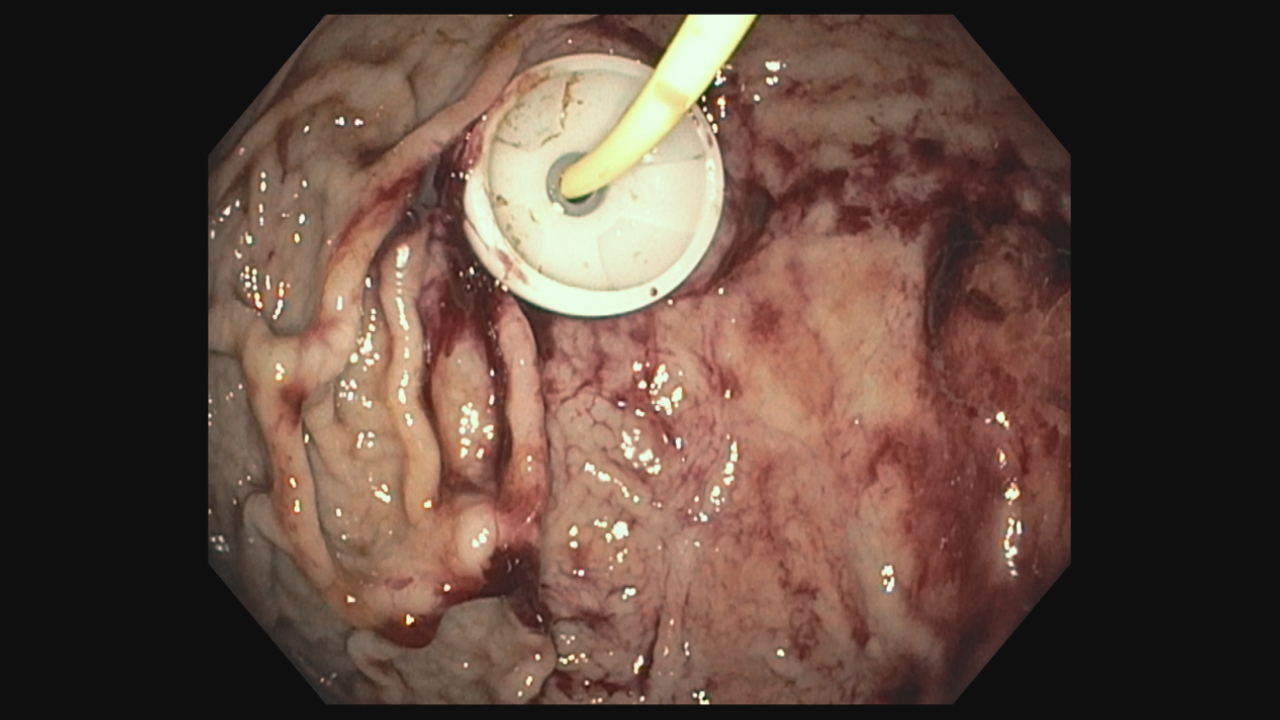
Methods: A 63-year-old male with Atrial Fibrillation (on apixaban, held 48 hours pre-procedure), duodenal obstruction, and perihepatic abscess underwent PEG-J placement via the Ponsky pull technique for enteral access. A 20 Fr MIC gastrostomy tube with a 14Fr jejunal extension (Avanos Medical Inc.) was inserted uneventfully, with self-limited endoscopic oozing at the gastric puncture site (Image 1). Twelve hours post-procedure, hemoglobin dropped acutely from 10.8 to 6.7 g/dL, accompanied by hemodynamic instability. Aspiration of sanguineous fluid via the PEG tube prompted computed tomography angiography (CTA), revealing transection of a tortuous right gastroepiploic artery (Image 2). Interventional Radiology (IR) embolization was attempted but hypertrophy of the inferior pancreaticoduodenal artery with marked tortuosity of collateral vessels resulted in inability to access the transected gastroepiploic artery. Emergent laparotomy confirmed active bleeding from the transected vessel with greater curvature ischemia, necessitating partial gastrectomy and direct surgical jejunostomy. The patient recovered without further complications. Discussion: This case illustrates an uncommon early postoperative complication of PEG tube placement. Intrabdominal inflammation likely contributed to the hypertrophied gastroduodenal artery which was transected at the time of trocar insertion. Vigilant monitoring, low threshold for further investigation and multidisciplinary collaboration are needed in high-risk patients.
Figure: PEG tube placement site showing mild oozing.
Figure: CTA (Computed Tomography Angiography) showing the G tube (blue arrows) transecting through the right gastro-epiploic artery (orange dotted line).
Disclosures: Ashwariya Ohri indicated no relevant financial relationships. Preeyati Chopra indicated no relevant financial relationships. Mayank Goyal indicated no relevant financial relationships. Dave Buttar indicated no relevant financial relationships. Manik Aggarwal indicated no relevant financial relationships. Nayantara Coelho-Prabhu indicated no relevant financial relationships.
Ashwariya Ohri, MBBS1, Preeyati Chopra, MBBS2, Mayank Goyal, MBBS3, Dave Buttar, MBBS3, Manik Aggarwal, MD3, Nayantara Coelho-Prabhu, MBBS, FACG3. P5758 - Intraperitoneal Hemorrhage Following PEG Tube Insertion: Recognition and Management of a Rare but Life-Threatening Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.