Dinkar Ahuja, MD1, Mohammed Abourahma, MD2, Kartik Devgan, MD1, Emma Schnittka, DO3, Alexander O'Hara, MD3, Rohit Agrawal, MD1 1Loyola University Medical Center, Chicago, IL; 2Loyola University Medical Center, Willowbrook, IL; 3Loyola University Medical Center, Maywood, IL Introduction: Obesity is a growing pandemic with prevalence doubling in 70 countries since 1980. The rise in obesity has led to increased bariatric procedures such as Roux-en-Y Gastric Bypass (RYGB). Endoscopic evaluation of the excluded stomach and duodenum in RYGB is challenging with device assisted enteroscopy, which has a technical and clinical failure rate up to 30%. Endoscopic ultrasound (EUS) directed transgastric ERCP (EDGE) utilizes lumen apposing metal stents (LAMS) to create a fistula and access the excluded stomach. This technique is popular for pancreaticobiliary access but underutilized for benign pathologies. Through our case series we report use of EUS guided gastro-gastrostomy (EGG) for managing recurrent GI bleeding and gastric outlet obstruction (GOO) of the excluded stomach.
Case Description/
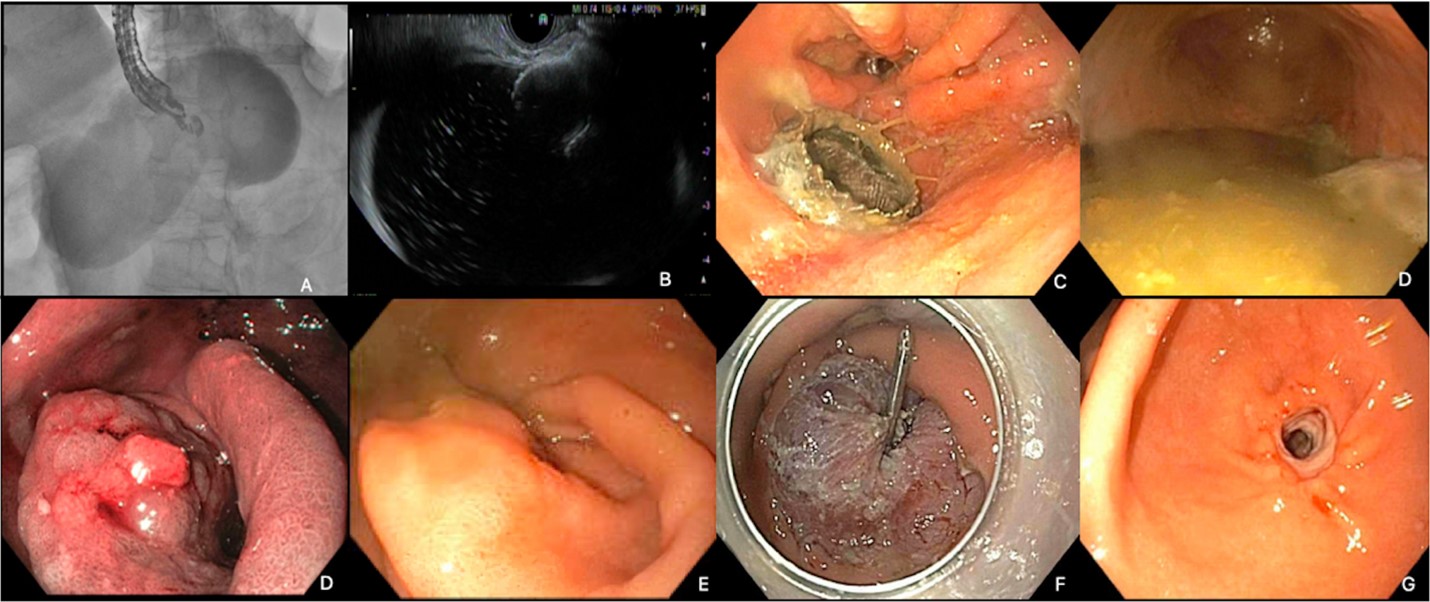
Methods: A 78-year-old female with prior RYGB presented with abdominal pain and distension. CT revealed a pyloric mass causing GOO of the excluded stomach. EGG was performed; follow up EGD via LAMS showed a large hyperplastic polyp from antrum to pylorus. Due to pyloric stenosis, only an ultraslim scope could traverse. A venting PEG was placed for symptom relief. EMR of a large circumferential polyp was performed. Three weeks later, EGD showed a healing ulcer with resolution of stenosis. The pylorus was dilated to 12 mm, PEG removed, and LAMS left in place for continued monitoring. (Figure 1)
In another case, a 70-year-old male with prior RYGB and recurrent GI bleed presented with melena. Repeat EGD revealed two large inflammatory polyps in the gastric pouch, which were resected. Three weeks later, he re-presented with melena; EGD showed healed EMR sites with no active bleeding. Given prior CT showing contrast extravasation in the excluded stomach, EGG was performed; subsequent EGD showed no excluded stomach or pancreatobiliary abnormalities. Capsule endoscopy via the gastro-gastric fistula suggested a possible lower GI bleed, but repeat colonoscopy was unremarkable. The LAMS was removed after completion of workup. (Figure 2) Discussion: Utility of EGG to facilitate EDGE has been established. This case series demonstrates the advantages of EGG over device assisted enteroscopy for diagnostic and therapeutic purposes. While concerns persist regarding the potential reversal of the bariatric benefits of RYGB with EGG, retrospective studies show spontaneous fistula closure in over 90% of cases within 2 months. We propose EGG as a broadly applicable technique for managing benign conditions in RYGB patients.
Figure: Figure 1: Gastro-gastrostomy utilizing lumen apposing metal stent (A, B, C); Multilobulated polyp obstructing pylorus leading to gastric outlet obstruction (D, E, F); Gastric mucosa after EMR of large obstructing polyp (F); Resolved pyloric stenosis (G)
Figure: Figure 2: Gastro-gastrostomy utilizing lumen apposing metal stent (A); Excluded gastric mucosa without evidence of recent hemorrhage (B); Video capsule endoscopy showing large bowel bleed (C)
Disclosures: Dinkar Ahuja indicated no relevant financial relationships. Mohammed Abourahma indicated no relevant financial relationships. Kartik Devgan indicated no relevant financial relationships. Emma Schnittka indicated no relevant financial relationships. Alexander O'Hara indicated no relevant financial relationships. Rohit Agrawal indicated no relevant financial relationships.
Dinkar Ahuja, MD1, Mohammed Abourahma, MD2, Kartik Devgan, MD1, Emma Schnittka, DO3, Alexander O'Hara, MD3, Rohit Agrawal, MD1. P5726 - Innovative Use of EUS-Guided Gastro-Gastrostomy in Roux-en-Y Gastric Bypass Patients for Management of Benign Pathologies, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.