Seunghee Han, MBChB1, Srikar Reddy, MD2 1MedStar Health, Baltimore, MD; 2MedStar Georgetown University Hospital, Washington, DC Introduction: Transjugular intrahepatic portosystemic shunt (TIPS) placement is a well-established intervention for managing complications of portal hypertension, including refractory ascites and variceal bleeding. While TIPS-related infections are rare, recurrent episodes should prompt investigation for structural complications. We present a unique case of recurrent TIPS-associated infection caused by a fistulous connection between the TIPS and biliary tree—an exceedingly rare and underreported complication.
Case Description/
Methods: A 33-year-old man with chronic portal vein thrombosis due to homozygous MTHFR mutation and a history of TIPS placement (2/2020) for portal hypertension presented with fever, abdominal pain, emesis, and diarrhea. He had a history of recurrent TIPS-associated infections (TIPSitis) beginning 8 months post-placement, despite chronic antibiotic suppression and multiple TIPS revisions (12/2020, 1/2021, 4/2025). He also required biliary stenting for obstruction from venous collaterals. Blood cultures across hospitalizations grew Streptococcus viridans, Citrobacter, Enterococcus faecalis, and Candida species. Prior ERCP in 3/2024 raised concern for a TIPS–biliary fistula, though contrast extravasation was not seen. During this admission, MRCP revealed an occluded TIPS and biliary dilation near a suspected erosion site. ERCP confirmed contrast extravasation from the biliary tree into the TIPS. A fully covered metal stent was placed as a temporizing measure while he underwent evaluation for multivisceral transplantation. He later died from an upper GI bleed. Discussion: TIPS–biliary fistula is an exceptionally rare but serious complication, with only three similar cases reported—all requiring transplantation. These fistulas provide a persistent route for microbial translocation, leading to recurrent infections refractory to antibiotics. While fistula formation may occur acutely due to bile duct injury, delayed onset is likely related to stent-induced pressure necrosis or ischemia from thrombosis and repeated revisions. No standardized treatment exists; covered stent placement may offer temporary control. In patients with recurrent, polymicrobial, or fungal TIPSitis, clinicians should maintain high suspicion for TIPS–biliary fistula. Early recognition is key to guide timely intervention and consideration for transplant.
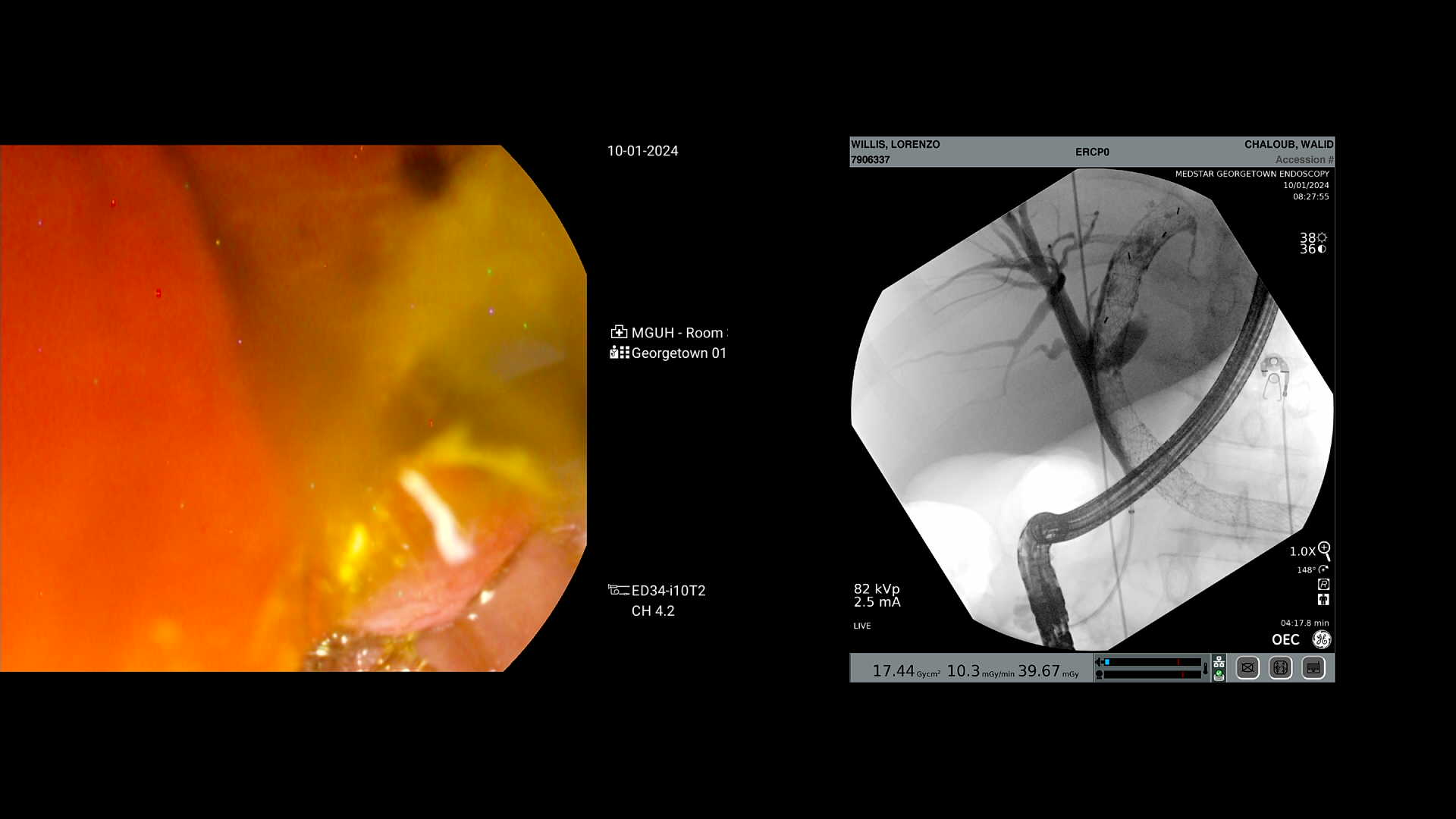
Figure: ERCP image showing contrast extravasation from biliary tree to TIPS.
Disclosures: Seunghee Han indicated no relevant financial relationships. Srikar Reddy indicated no relevant financial relationships.
Seunghee Han, MBChB1, Srikar Reddy, MD2. P5709 - Fatal Outcome of a Rare TIPS-Biliary Fistula: Lessons From Recurrent Infection, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.