Ujasbhai Patel, MD1, Kshitij Thakur, MD2, Rebecca Aquino, MD1 1University of Kentucky College of Medicine, Lexington, KY; 2University of Kentucky, Lexington, KY Introduction: A 61 year old female with history of decompensated hepatitis C cirrhosis with liver transplant in 2005 followed by repeat transplantation due to recurrence of hepatitis C in 2014 with care complicated by anastomotic strictures requiring repeat ERCP with stenting and stent exchanges presented for routine outpatient exchange.
Case Description/
Methods: ERCP revealed a mid-common bile duct anastomotic stricture with the goal of bridging the stricture with WallFlex fully covered metal stent. However, it was mis-deployed and lodged within the common bile duct (CBD). Multiple attempts were made for stent retrieval using standard removal techniques including rat-tooth forceps, pediatric biopsy forceps, standard biopsy forceps, and retrieval basket but the attempts were unsuccessful as the CBD was diffusely dilated adding further to the difficulty of the case. This resulted in instruments passing parallel to and beyond the stent. At this point, decision was made to perform cholangioscopy for direct visualization of the CBD. A digital cholangioscope was advanced over a guidewire into the distal CBD. A SpyBite™ biopsy forceps was used to grasp the stent under direct visualization. The stent was successfully dislodged and subsequently removed from the duct with rat-tooth forceps. The patient tolerated this procedure well and no additional intra-procedural and post-procedural complications were noted upon assessing the patient in recovery area. Discussion: This case highlights the adjunct of cholangioscopy usage by advanced interventional and therapeutic gastroenterologists in managing challenging biliary stent removals when conventional techniques are unsuccessful, particularly in post-transplant patients with altered anatomy or chronic strictures.This may prevent the need for more invasive surgical interventions.
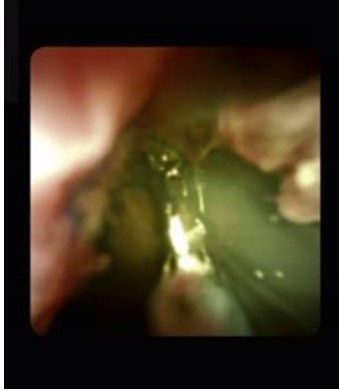
Figure: Cholangioscopy view of SpyBite grasping the WallFlex biliary stent.
Figure: Fluoroscopy view showing significantly dilated duct causing all stent removal instruments to pass adjacent to the stent.
Disclosures: Ujasbhai Patel indicated no relevant financial relationships. Kshitij Thakur indicated no relevant financial relationships. Rebecca Aquino indicated no relevant financial relationships.
Ujasbhai Patel, MD1, Kshitij Thakur, MD2, Rebecca Aquino, MD1. P5704 - Unconventional Method for the Removal of a Misdeployed Biliary WallFlex Stent U, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.