Khaled Alsabbagh Alchirazi, MD1, Nishkarsh Kumar, 2, Sahibzada Usman Latif, MD3 1Aurora Health Care, Brookfield, WI; 2St. Luke's Hospital, Milwaukee, WI; 3Aurora Healthcare, Milwaukee, WI Introduction: Enterolithiasis presenting as fecaliths is a rare but important complication of Crohn’s disease, particularly in patients with prior small bowel resection or stricturing disease. Often seen as fecalith on imaging it can lead to bowel obstruction, perforation and stercoral ulcerations in stone bed. Obstructive fecaliths in the setting of Crohn’s-related strictures can mimic or exacerbate disease flare and require a high index of suspicion and tailored endoscopic intervention.
Case Description/
Methods: A 66-year-old male with a history of stricturing and penetrating Crohn’s disease complicated by small bowel fistulas and ileocolonic stricture requiring partial ileo-colectomy had disease recurrence at anastomosis. Was eventually able to achieve clinical and endoscopic remission with aggressive biologic therapy but developed anastomotic stricture. Presented with abdominal pain, nausea, and obstipation symptoms. CT scan of abdomen/pelvis showed multiple calcified fecaliths proximal to the ileo-colonic anastomosis with proximal dilation of the bowel. These findings were suggestive of slow transit and possible obstructive fecaliths at the anastomotic site. Colonoscopy revealed a high-grade pin hole stricture at the ileo-colonic anastomosis without any active disease. Fluroscopic guided graded balloon stricturoplasty was performed with extraction of multiple obstructive fecaliths. Procedure had to be repeated over a few sessions for complete evacuation of fecaliths and serial dilation of the anastomotic stricture. Patient has done well with non-surgical management and close follow-up Discussion: Stasis of intestinal contents with continued absorptions of the fluid component leads to enterolithiasis. Crohn’s disease related stricturing can sometimes lead to development of fecaliths. This case illustrates an uncommon cause of intestinal obstruction in Crohn’s disease caused by fecalith impaction at the surgical anastomotic stricture. CT imaging provided early suspicion and differentiation from disease exacerbation. Advancements in endoscopic therapy such as balloon stricturoplasty, needle knife stricturotomy and fecalith extraction allows for non- surgical management in these patients. Clinicians should maintain a high index of suspicion for this relatively rare entity, especially in patients with altered surgical anatomy and delayed transit.
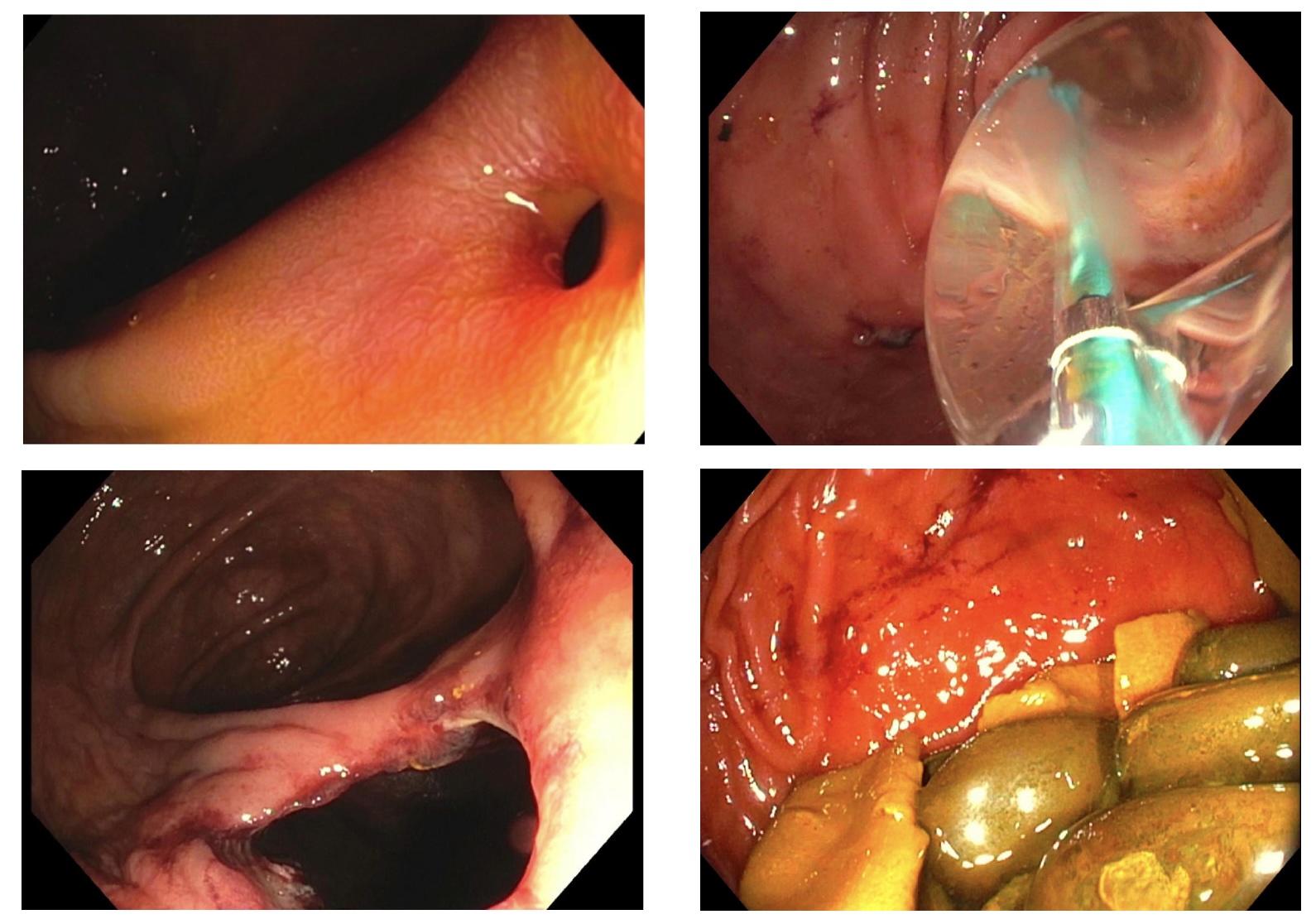
Figure: Endoscopic management of ileocolonic anastomotic stricture: (Top left) visualization of the stricture at the ileocecal (IC) valve anastomosis; (Top right) balloon dilatation performed for stricturoplasty; (Bottom left) post-dilation view showing improved luminal patency; (Bottom right) removal of impacted stool stones and debris from the proximal bowel.
Disclosures: Khaled Alsabbagh Alchirazi indicated no relevant financial relationships. Nishkarsh Kumar indicated no relevant financial relationships. Sahibzada Usman Latif indicated no relevant financial relationships.
Khaled Alsabbagh Alchirazi, MD1, Nishkarsh Kumar, 2, Sahibzada Usman Latif, MD3. P5703 - Chronic Crohn’s Stricture: A Hotbed for Obstructing Fecaliths, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.