P5702 - EUS-Directed Transgastric ERCP With Cholangioscopy for the Management of Biliary Anastomotic Stricture in a Living Donor Liver Transplant Recipient
University of South Florida Morsani College of Medicine Tampa, FL
Award: ACG Presidential Poster Award
Quinten Federico, MD1, Pratik Patel, MD2, Pushpak Taunk, MD1 1University of South Florida Morsani College of Medicine, Tampa, FL; 2USF Health, Tampa, FL Introduction: Surgically altered foregut anatomy can prohibit standard Endoscopic Retrograde Cholangiopancreatography (ERCP) techniques. The EUS-Directed Transgastric ERCP (EDGE) procedure has dramatically improved management of biliary disorders in these patients. Limited data exists in the use of EDGE for the management of biliary anastomotic strictures. Incidence of both liver transplantation (LT) and gastric bypass have increased over the years, making this event more frequent. To the best of our knowledge, we present the first reported case of single-session EDGE with the use of cholangioscopy for the management of severe anastomotic biliary stricture in a living donor LT recipient.
Case Description/
Methods: A 43-year-old female with a history of Roux-en-Y Gastric Bypass (RNYGB) and living donor LT for alcohol-associated liver disease initially presented to our clinic with asymptomatic liver enzyme elevations; AST 202, ALT 101, ALP 561, and T bili 1.3. MRCP imaging revealed a high-grade narrowing at the hepatic duct confluence with intrahepatic biliary duct dilation, indicative of a severe biliary anastomotic stricture. Initial balloon-assisted ERCP was unsuccessful, but a single-session EDGE was subsequently performed. Cholangiogram revealed a severe anastomotic stricture, with inability for biliary guidewire to traverse the stenosis. Using cholangioscopy, the anastomosis was located and a 0.025-inch guidewire was used to traverse the stricture. Balloon dilation of the stricture was performed to 4 mm and a 10 Fr plastic biliary stent was placed. Repeat ERCP, 6 weeks later, involved placement of multiple plastic stents. Final ERCP, 3 months after initial EDGE, showed resolution of the anastomotic stricture, with removal of the lumen apposing metal stent, and normalization of liver enzymes. Discussion: In 2014, EDGE first provided an alternative to balloon-assisted ERCP, laparoscopic-assisted ERCP, and percutaneous biliary decompression in patients with RNYGB, a procedure more common the past few decades. Similarly, there has been a greater than 70% rise in LT volume compared to the previous decade. While the EDGE procedure has been described in post-LT patients, the use of cholangioscopy in a living donor transplant recipient has not been described. While weight gain is a common concern post-EDGE in this population, recent studies suggest no significant weight gain occurs. Given this, the EDGE procedure appears to be a viable option for the management of biliary complications in post-LT patients.
Figure: Cholangiogram displaying patient’s severe anastomotic stricture
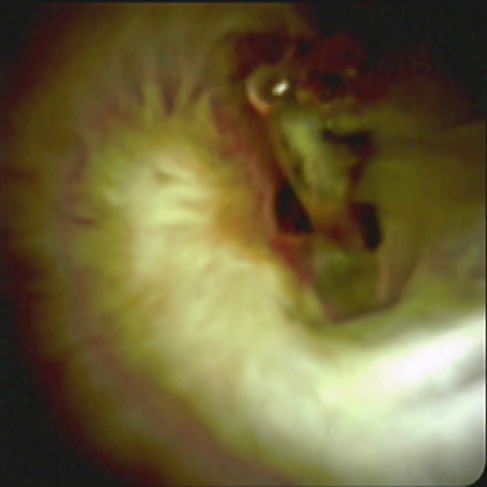
Figure: Cholangioscopy of Biliary Anastomotic Stricture
Disclosures: Quinten Federico indicated no relevant financial relationships. Pratik Patel indicated no relevant financial relationships. Pushpak Taunk: Boston Scientific – Consultant. Endo Therapeutics – Consultant. Neptune Medical – Consultant.
Quinten Federico, MD1, Pratik Patel, MD2, Pushpak Taunk, MD1. P5702 - EUS-Directed Transgastric ERCP With Cholangioscopy for the Management of Biliary Anastomotic Stricture in a Living Donor Liver Transplant Recipient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")