P5682 - Endoscopic Full-Thickness Resection (EFTR): A 5-Year Study at a Tertiary Regional Medical Center, Clinical Indications, Outcomes, and Procedural Insights
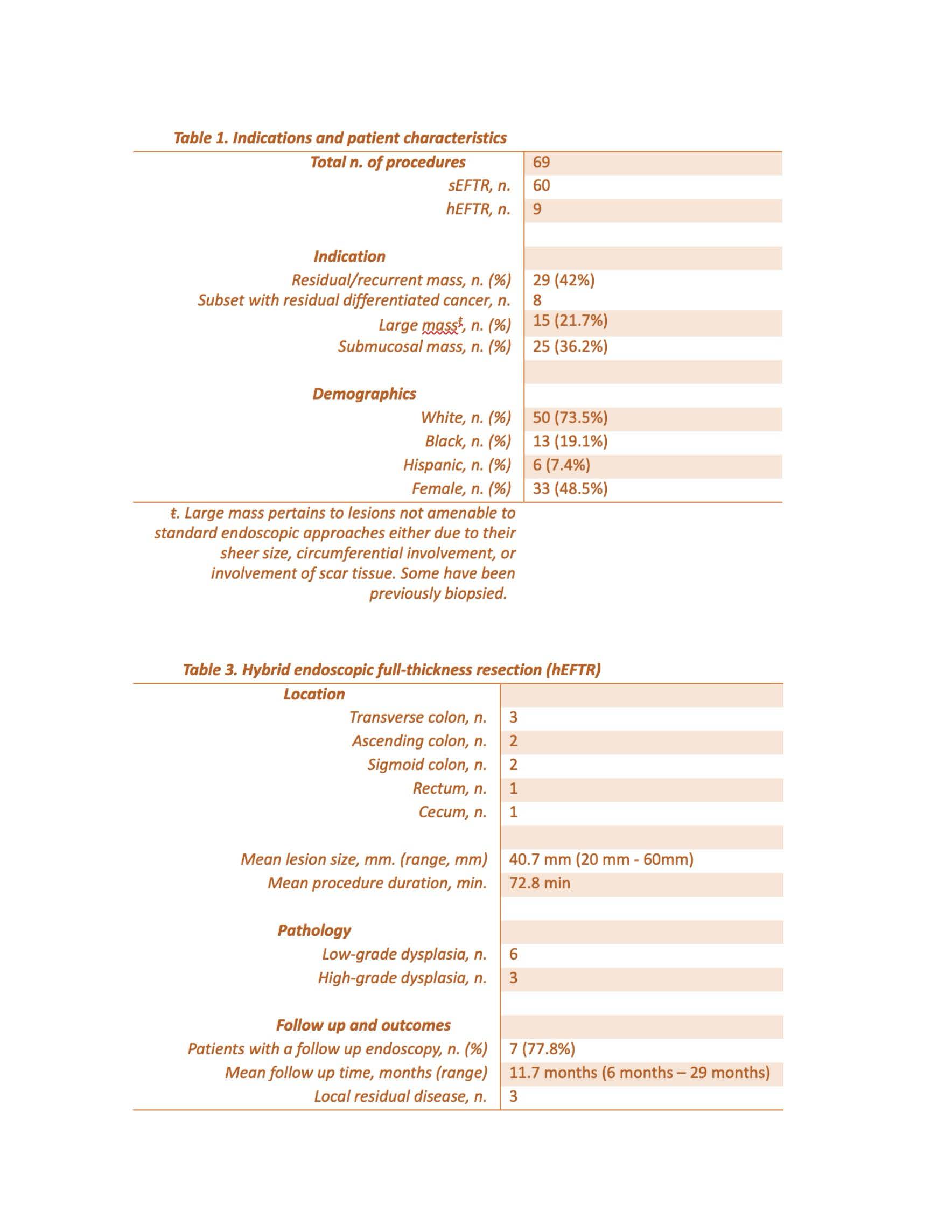
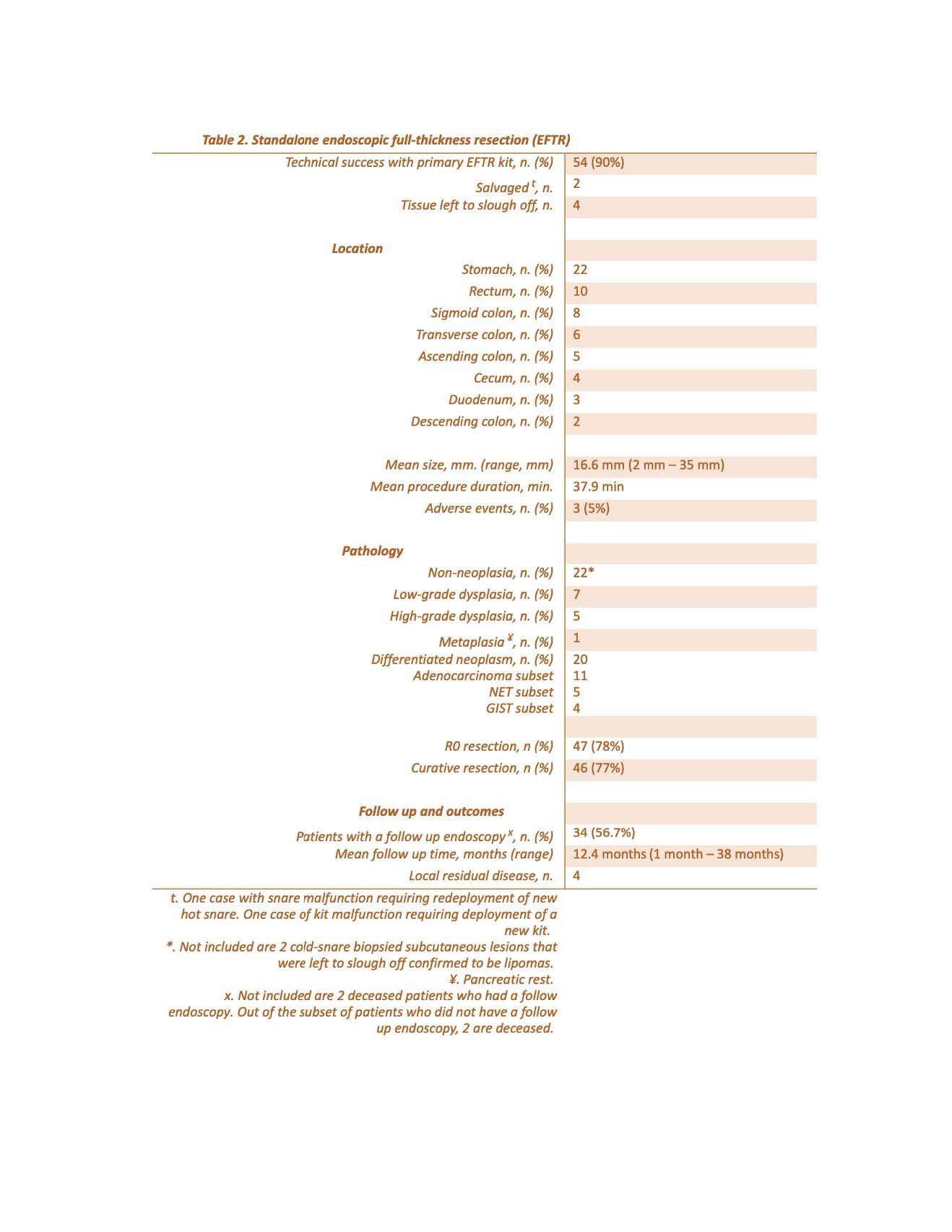
Yuriy Kotsurovskyy, MD1, Khaled Alsabbagh Alchirazi, MD2, Meklit Hunde, MD1, Nishkarsh Kumar, 3, Mohammad Aasim Khan, MBBS4, Sahibzada Usman Latif, MD1 1Aurora Healthcare, Milwaukee, WI; 2Aurora Health Care, Brookfield, WI; 3St. Luke's Hospital, Milwaukee, WI; 4MBBS, CBPSD, Milwaukee, WI Introduction: Endoscopic full-thickness resection (EFTR) is an emerging technique for the management of complex gastrointestinal lesions not amenable to standard endoscopic methods. This study presents data from the largest tertiary care center in Wisconsin over the last 5 years, comparing standalone EFTR (sEFTR) and hybrid EFTR (hEFTR) approaches, with a focus on procedural outcomes, lesion characteristics, and longitudinal follow-up data. Methods: A retrospective analysis was conducted on 69 EFTR procedures (sEFTR: n=60; hEFTR: n=9) performed at a tertiary care center 2021-2025. Indications included residual/recurrent lesions, submucosal tumors, and large or fibrotic lesions. Data on demographics, lesion location, pathology, procedure duration, and outcomes were collected Results: A total of 69 EFTRs were performed from 2021–2025 (sEFTR: n=60; hEFTR: n=9). Indications included residual/recurrent lesions (42%), submucosal tumors, and large or fibrotic lesions (21.7% sized 20–60 mm). Most patients were White (73.5%), with near-equal gender distribution (48.5% female). In the sEFTR group, the stomach (n=22) and rectum (n=10) were most common. Mean lesion size was 16.6 mm (range: 2–35 mm), mean procedure time 37.9 minutes. Technical success with the primary EFTR kit was 90%, with 5% adverse events. R0 and curative resection rates were 78% and 77%, respectively. Pathologies included non-neoplasia (n=22), differentiated neoplasia (n=20), and low-/high-grade dysplasia (n=12). Among 34 patients (56.7%) with follow-up (mean: 12.4 months), 4 had local residual disease. The hEFTR group mainly targeted transverse (n=3) and ascending (n=2) colon lesions, with larger mean lesion size (40.7 mm) and longer mean procedure time (72.8 minutes). Pathology revealed low-grade dysplasia (n=6) and high-grade dysplasia (n=3). Of 7 patients with follow-up (77.8%), 3 had local residual disease (mean: 11.7 months) Discussion: EFTR is a safe and effective for managing challenging GI lesions, with high technical and curative resection rates. sEFTR is more commonly utilized and efficient for smaller lesions, particularly in the upper GI tract. hEFTR plays an important role in larger or fibrotic colonic lesions. Close endoscopic follow-up remains essential due to the risk of local residual disease. Our experience is based on a large volume tertiary care referral center with expertise in advanced endoscopic techniques and surgical back-up. Endoscopist’s technical expertise is essential for this technique with a sharp learning curve.
Disclosures: Yuriy Kotsurovskyy indicated no relevant financial relationships. Khaled Alsabbagh Alchirazi indicated no relevant financial relationships. Meklit Hunde indicated no relevant financial relationships. Nishkarsh Kumar indicated no relevant financial relationships. Mohammad Aasim Khan indicated no relevant financial relationships. Sahibzada Usman Latif indicated no relevant financial relationships.
Yuriy Kotsurovskyy, MD1, Khaled Alsabbagh Alchirazi, MD2, Meklit Hunde, MD1, Nishkarsh Kumar, 3, Mohammad Aasim Khan, MBBS4, Sahibzada Usman Latif, MD1. P5682 - Endoscopic Full-Thickness Resection (EFTR): A 5-Year Study at a Tertiary Regional Medical Center, Clinical Indications, Outcomes, and Procedural Insights, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.