P5646 - Comparative Risk of Post-Endoscopic Dilation Outcomes in Patients on Dual vs Single Antiplatelet Therapy: A Propensity-Matched Analysis From a Global Real-World Dataset
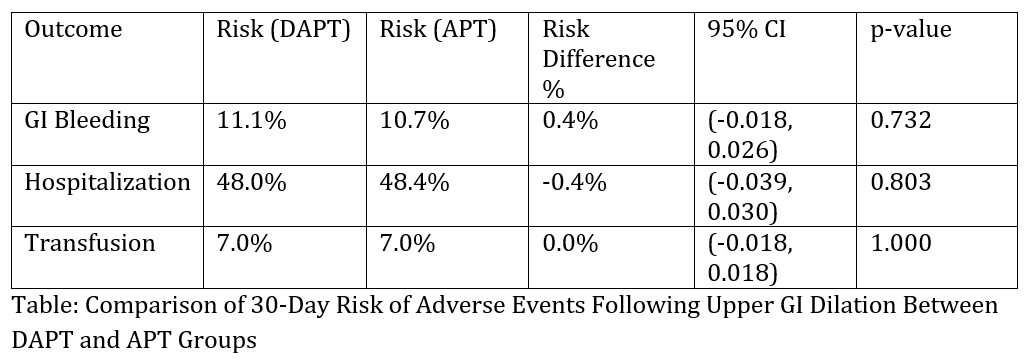
Osama Alshakhatreh, MD1, Omar Arman, MD, MPH2, Shamayel Safdar, MBBS1, Ibrahim Mohammed, MD1, Seth Richter, MD, FACG1 1Albany Medical Center, Albany, NY; 2University at Buffalo, Buffalo, NY Introduction: Endoscopic dilation of upper gastrointestinal strictures is performed in patients with benign or malignant conditions. Single antiplatelet therapy (APT) is a known risk factor for bleeding, but data is limited on whether dual antiplatelet therapy (DAPT) confers a higher risk of adverse outcomes compared to single APT in this context. We aim to compare the 30-day post-procedural outcomes in patients on DAPT versus APT using a large real-world database. Methods: A retrospective cohort analysis was performed using the TriNetX Global Collaborative Network. Adults (≥18 years) who underwent upper GI endoscopic dilation and were on either DAPT (aspirin plus clopidogrel or prasugrel or ticagrelor) or single APT (aspirin or a P2Y12 inhibitor) within 7 days before the procedure were included. Patients on anticoagulants were excluded. Propensity score matching (1:1) was performed to match baseline demographics and comorbidities, and PPI use. The primary outcomes were 30-day risks of GI bleeding, hospitalization, and transfusion. Falsification endpoints were included to assess for residual confounding. Risk differences (RD) between groups were reported with 95% confidence intervals (CI). Results: A total of 3,156 patients (1,578 in each group) were included after propensity score matching. The 30-day risk of GI bleeding was 11.1% in the DAPT group compared to 10.7% in the APT group, with a risk difference of 0.4% (95% CI: -1.8% to 2.6%; p = 0.732). Hospitalization occurred in 48.0% of patients on DAPT versus 48.4% on APT, with a risk difference of -0.4% (95% CI: -3.9% to 3.0%; p = 0.803). The risk of transfusion was identical between groups at 7.0%, resulting in a risk difference of 0.0% (95% CI: -1.8% to 1.8%; p = 1.000). Discussion: In this large, real-world, propensity-matched analysis, DAPT was not associated with significantly higher 30-day risk of GI bleeding, hospitalization, or transfusion compared to APT following endoscopic dilation. These findings suggest that routine interruption or modification of DAPT may not be necessary in patients at high thrombotic risk undergoing necessary upper GI dilation.
Figure: Table: Comparison of 30-Day Risk of Adverse Events Following Upper GI Dilation Between DAPT and APT Groups
Disclosures: Osama Alshakhatreh indicated no relevant financial relationships. Omar Arman indicated no relevant financial relationships. Shamayel Safdar indicated no relevant financial relationships. Ibrahim Mohammed indicated no relevant financial relationships. Seth Richter indicated no relevant financial relationships.
Osama Alshakhatreh, MD1, Omar Arman, MD, MPH2, Shamayel Safdar, MBBS1, Ibrahim Mohammed, MD1, Seth Richter, MD, FACG1. P5646 - Comparative Risk of Post-Endoscopic Dilation Outcomes in Patients on Dual vs Single Antiplatelet Therapy: A Propensity-Matched Analysis From a Global Real-World Dataset, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.