Kyle S. Hamann, DO1, Charles Swanson, DO2, Ashish Shah, MD3, Michael Anderson, MD2 1Riverside Medical Center, Lemont, IL; 2Riverside Medical Center, Kankakee, IL; 3Digestive Disease Consultants, Bourbonnais, IL Introduction: Herpes Zoster epiglottitis is an exceedingly rare diagnosis with a paucity of biopsy-proven cases in the medical literature. Although uncommon, not properly diagnosing and promptly treating Herpes Zoster epiglottitis can lead to chronic dysphagia, recurrent superimposed bacterial infections, and cranial nerve abnormalities [3].
Case Description/
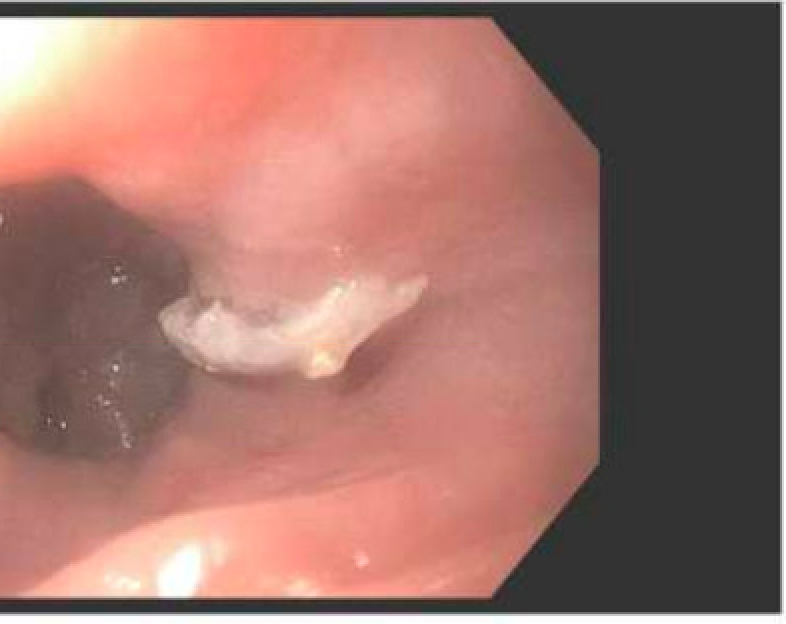
Methods: We present a 74-year-old immunocompetent male initially presented to the Emergency Department (ED) from a VA nursing home due to dysphagia and inability to tolerate secretions. The patient was hospitalized roughly one week prior for a similar issue which did temporarily improve with steroids. Cranial nerve evaluation on presentation was unremarkable. CT soft tissue neck with contrast was obtained demonstrating asymmetric epiglottis thickening right of midline. ENT was consulted and laryngoscopy was performed with direct visualization of white plaques along with ulcerations lining the left lingual surface of the epiglottis and copious purulent secretions. Supraglottic edema was also visualized. The patient was started empirically on IV Acyclovir, Fluconazole, Ceftriaxone, and Flagyl. Gastroenterology was consulted. Joint procedure with repeat laryngoscopy and esophagogastroduodenoscopy (EGD) with biopsy was completed. On the EGD portion, pus was noted to the back of the oropharynx with white plaques in the esophagus. No ulcerations were noted and biopsies were taken. On the laryngoscopy portion, left supraglottic edema and white plaque lesions were visualized. Tissue biopsy results from EGD did confirm Herpes Zoster esophagitis, epiglottitis, and laryngitis. The patient did have improvement in pain and secretion tolerance with IV Acyclovir. Antibiotics were discontinued and he was discharged home on Valtrex. There was no dysphagia or odynophagia noted on follow up appointment one month later. Discussion: Adult cases of epiglottis are a rare phenomenon occurring in one out of every 100,000 people annually. It was previously assumed that epiglottitis derived from viral etiology did not exist and all presumed instances were due to secondary bacterial infections with H Influenza type b accounting for over 90% of instances [1]. It has also been estimated that roughly 70% of patients affected with Herpes Zoster laryngitis are concurrently immunocompromised [2]. There have been reported findings of biopsy proven VZV epiglottitis in the order of single digits making this an exceedingly rare diagnostic finding especially in an immunocompetent host.
Figure: Esophageal Herpetic Plaques
Disclosures: Kyle Hamann indicated no relevant financial relationships. Charles Swanson indicated no relevant financial relationships. Ashish Shah indicated no relevant financial relationships. Michael Anderson indicated no relevant financial relationships.
Kyle S. Hamann, DO1, Charles Swanson, DO2, Ashish Shah, MD3, Michael Anderson, MD2. P5623 - Epiglottitis of an Unusual Etiology, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.