University of British Columbia Department of Medicine Surrey, BC, Canada
Bachviet AH. Nguyen, MD1, Astrid-Jane Williams, MD2, Yvette Leung, MD2 1University of British Columbia Department of Medicine, Surrey, BC, Canada; 2UBC Department of Medicine/IBD Centre of BC, Vancouver, BC, Canada Introduction: Cytomegalovirus (CMV) is a double-stranded DNA virus transmitted via bodily fluids that is associated with a variety of clinical manifestations. Immunocompetent hosts tend to be asymptomatic while immunocompromised hosts present with more severe CMV infection, such as retinitis, pneumonitis, hepatitis and colitis.
We present the case of an immunocompetent patient with severe CMV colitis and hepatitis.
Case Description/
Methods: A 55 year old lady with a remote history of Graves disease presented to the emergency room with a 6 day history of intermittent diffuse abdominal cramping, nausea/vomiting, severe fatigue, anorexia, and non-bloody diarrhea. There was diffuse periumbilical tenderness without signs of peritonitis on palpation with the remainder of her physical exam being unremarkable.
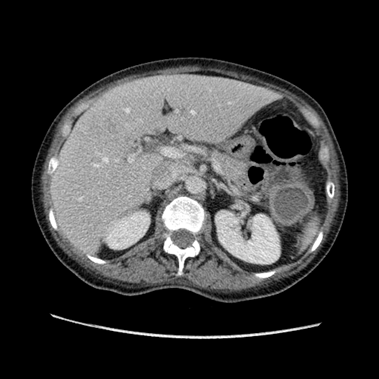
Her bloodwork demonstrated leukocytosis and severe hepatitis with a negative infectious work-up. Cytomegalovirus (CMV) IgG was positive. A CT abdomen-pelvis with intravenous contrast revealed small low-density lesions in the liver and left colonic circumferential wall thickening from the splenic flexure to the rectosigmoid colon.
The severe hepatitis self-resolved but she then developed hematochezia. A flexible sigmoidoscopy with biopsy noted left-sided rectal-sparing colitis with ulcers and a positive CMV immunostain. Repeat CMV serology was now positive for both IgM and IgG with a high viral DNA load. With steroid use (intravenous then oral) and valganciclovir, her abdominal pain and diarrhea improved. Repeat follow-up colonoscopies with biopsy within the following 12 months demonstrated resolution of active colitis and negative CMV immunostain without changes suggestive of inflammatory bowel disease (IBD). An immunodeficiency work-up was negative. Discussion: We present the rare case of CMV colitis and hepatitis in an immunocompetent host without an underlying predisposing chronic illness such as IBD.
The differential diagnosis for severe colitis with rectal sparing includes infectious colitis, Crohn's disease (CD), and ischemic colitis. The involved segment of colon was regarded too extensive for ischemic colitis while subsequent endoscopic assessment did not suggest CD.
The diagnosis of CMV colitis should be considered in an immunocompetent patient after excluding more common causes of diarrhea and if CMV confirmed, exclusion of an underlying immunodeficiency. Given the association between IBD and CMV infection, the possibility of a new diagnosis of IBD should also be investigated.
Figure: Figure 1: Initial CT abdo-pelvis demonstrating a thick-walled segment of colon extending from roughly the splenic flexure down to the junction of sigmoid colon suggestive of diffuse colitis.
Figure: Figure 2: Several low-density lesions identified in the liver on CT scan in the context of an acute CMV-associated hepatitis.
Disclosures: Bachviet Nguyen indicated no relevant financial relationships. Astrid-Jane Williams indicated no relevant financial relationships. Yvette Leung indicated no relevant financial relationships.
Bachviet AH. Nguyen, MD1, Astrid-Jane Williams, MD2, Yvette Leung, MD2. P5599 - A Rare Case of Acute Cytomegalovirus Colitis and Hepatitis in an Immunocompetent Host, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Bachviet AH Nguyen, MD (he/him/his) photo")