Jose Nunez Morales, 1, Raul Rios De Choudens, 2, Bianca Goyco Cortes, 2, Diego Roman-Colon, 2, Carla Cepero-Jimenez, 2, Andres Rabell-Bernal, 2, Jose Martin-Ortiz, MD, FACG2 1VA Caribbean Healthcare System, Guaynabo, Puerto Rico; 2VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Abdominal pain is a common, non-specific complaint with a broad differential diagnosis. Parasitic infections, often overlooked, remain a significant cause of gastrointestinal symptoms, especially in endemic areas. Intestinal parasitic infections (IPIs) have become an essential global concern in developing countries. Hookworm infection, caused mainly by Necator americanus and Ancylostoma duodenale, can present with abdominal discomfort, nausea, vomiting, and diarrheas. An itchy rash precedes some cases. Here, we present a case of persistent abdominal pain that was found to be secondary to hookworm infection.
Case Description/
Methods: This is the case of a 35 y/o male patient without significant comorbidities who presented to ED due to abdominal pain with associated nausea. Pain was described as severe, epigastric, and worsened with meals, associated with soft stools. He referred frequent NSAID use, family history of Crohn’s disease (brother), and a prior episode of non-complicated diverticulitis. Denied previous endoscopic procedures. He presented an unremarkable physical exam. The initial CBC revealed leukocytosis with marked eosinophilia at 28%. Renal and liver chemistries were unremarkable. Amylase and lipase were within normal limits. ABD/Pelvic CT scan without contrast showed no abdominal pathology. In view of concerns for peptic ulcer disease, an upper endoscopy was performed that showed erosive gastritis and a normal duodenum. Since EGD findings did not correlate with patient symptoms and given a family history of IBD along with previous diverticulitis episodes, a colonoscopy was recommended. A colonoscopy revealed normal colonic mucosa, but numerous cylindrical, off-white worms were noted in the cecum; one of these was taken for microbiological evaluation, which confirmed the presence of hookworm. The patient was treated with albendazole 400mg PO daily for 3 days. On follow-up, the patient had a complete resolution of his symptoms. Discussion: This case highlights the importance of taking into consideration parasitic infections, such as hookworm, in the differential diagnosis of abdominal pain, predominantly in patients with risk factors. Prompt recognition and adequate management with antiparasitic therapy can lead to rapid clinical improvement and prevent complications such as iron-deficiency anemia. A high index of suspicion for parasitic infections in the appropriate clinical context is essential to ensure timely diagnosis and management.
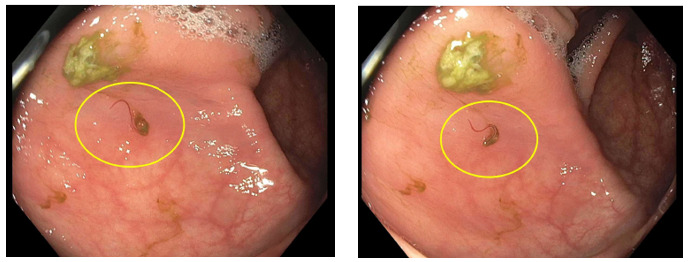
Figure: Figure 1. Colonoscopy images of cylindrical, off-white worms at cecum.
Disclosures: Jose Nunez Morales indicated no relevant financial relationships. Raul Rios De Choudens indicated no relevant financial relationships. Bianca Goyco Cortes indicated no relevant financial relationships. Diego Roman-Colon indicated no relevant financial relationships. Carla Cepero-Jimenez indicated no relevant financial relationships. Andres Rabell-Bernal indicated no relevant financial relationships. Jose Martin-Ortiz indicated no relevant financial relationships.
Jose Nunez Morales, 1, Raul Rios De Choudens, 2, Bianca Goyco Cortes, 2, Diego Roman-Colon, 2, Carla Cepero-Jimenez, 2, Andres Rabell-Bernal, 2, Jose Martin-Ortiz, MD, FACG2. P5594 - The Hidden Culprit: Abdominal Pain Secondary to Parasitic Infection, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.