University of Arizona College of Medicine Tucson, AZ
Maxwell Hart, MD1, Samuel Cheong, DO1, Rolando J. Leal, MD2 1University of Arizona College of Medicine, Tucson, AZ; 2Banner University Medical Center, Tucson, AZ Introduction: Hepatic hydrothorax refers to a pleural effusion in a patient with cirrhosis in the absence of other underlying cause and occurs in 5-15% of patient with cirrhosis. Diaphragmatic defects, more often found on the right, are thought to allow passage of ascites in to the pleural space. Similar to spontaneous bacterial peritonitis (SBP), patients with hepatic hydrothorax may develop spontaneous bacterial empyema (SBEM) as a result of bacteria from the abdominal cavity seeding the pleural effusion.
Case Description/
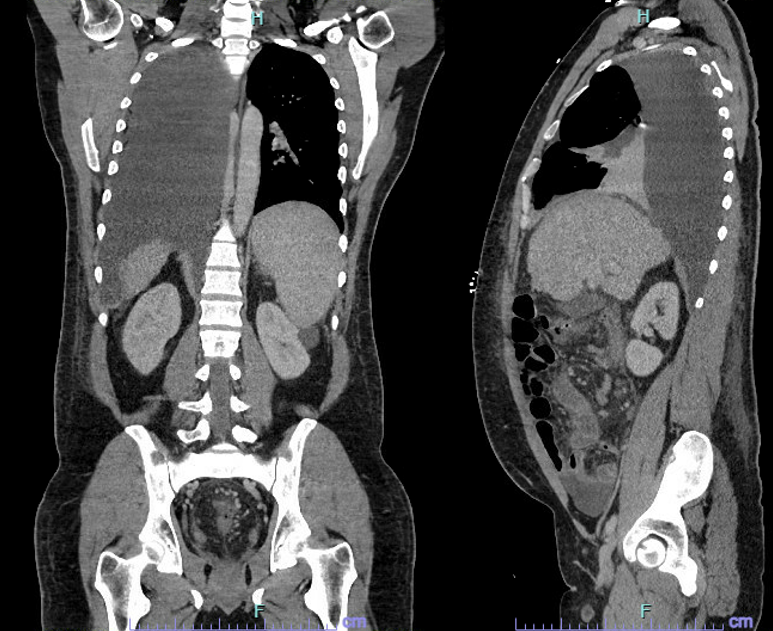
Methods: A 50-year-old man with no medical history presented with two weeks of dyspnea, abdominal distention, and fever. He reported drinking 6–8 beers daily for 20 years. Labs showed WBC 11.7, Hgb 12, Plt 131, Na 132, Cr 0.95, AST 102, ALT 63, alk phos 238, total bilirubin 7.4, INR 1.4, total protein 6.1, serum LDH 325. CT chest/abdomen/pelvis revealed a large right pleural effusion with compressive atelectasis and cirrhotic liver morphology, without ascites. Thoracentesis yielded 1,250cc of hazy yellow fluid: PMN 1,667, RBC 983, LDH 71, protein 0.7, negative cultures. Cirrhosis workup was otherwise unremarkable. He was diagnosed with SBEM and treated with IV ceftriaxone, transitioned to oral ciprofloxacin for outpatient prophylaxis. Over the next year, he developed hepatic encephalopathy and three episodes of recurrent C. difficile colitis requiring hospitalization. These were treated with vancomycin or fidaxomicin, and ultimately resolved after fecal microbiota transplant. He is now undergoing liver transplant evaluation. Discussion: SBEM has been described in 13-16% of patients with hepatic hydrothorax. The diagnostic criteria for SBEM are: positive pleural fluid culture and a PMN cell count >250 cells/mm3 OR negative pleural fluid culture and a PMN cell count >500 cells/mm3. No evidence of pneumonia on chest imaging is also a diagnostic criterion. Treatment of SBEM is the same as SBP, typically with a 3rd-generation cephalosporin, as well as furosemide and spironolactone when feasible. Prevention of SBEM has not been well studied, however we prescribed prophylactic ciprofloxacin as the patient would have otherwise met criteria for prophylaxis for SBP. Unfortunately this may have led to the development of C diff colitis. This case highlights an interesting presentation of cirrhosis in an undiagnosed patient as well as the potential consequences that prophylactic antibiotics may carry.
Figure: Figure 1
Disclosures: Maxwell Hart indicated no relevant financial relationships. Samuel Cheong indicated no relevant financial relationships. Rolando Leal indicated no relevant financial relationships.
Maxwell Hart, MD1, Samuel Cheong, DO1, Rolando J. Leal, MD2. P5592 - Empyema Unmasked: A Cirrhotic Tale With a <i>C. diff</i> Twist, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.