Denisa Horanlli, MD1, Fjona Tabaku, MD, MPH2, Suela Ristollari, MD3, Aida Haxhillari, MD4, Qirjako Gjino, MD5 1Pogradec Hospital, Albania, Korce, Korce, Albania; 2Mount Sinai Hospital Chicago, Chicago, IL; 3Pogradec Hospital, Albania, Pogradec, Korce, Albania; 4Korca Hospital, Albania, New York, NY; 5Korca Hospital, Albania, Korce, Korce, Albania Introduction: Crohn's disease (CD) is a transmural inflammatory process that can affect any segment of the gastrointestinal tract. It mainly affects the small bowel, specifically the terminal ileum. Rarely, it has also been found in the upper gastrointestinal segment, such as the esophagus. In this case report, we describe a case of esophageal Crohn’s disease
Case Description/
Methods: A 17-year-old male patient presented with a high fever, two episodes of hematemesis, heartburn, odynophagia, and dysphagia. He had these concerns for three days. He had no history of any other medical condition or drug abuse. His parents describe a history of Kawasaki disease in childhood. Laboratory results show elevated C-reactive protein levels, ferritin, and alpha1 and alpha2 globulins. Hepatitis B, C, CMV, EBV, and HIV 162 were negative. Ig E levels were normal.
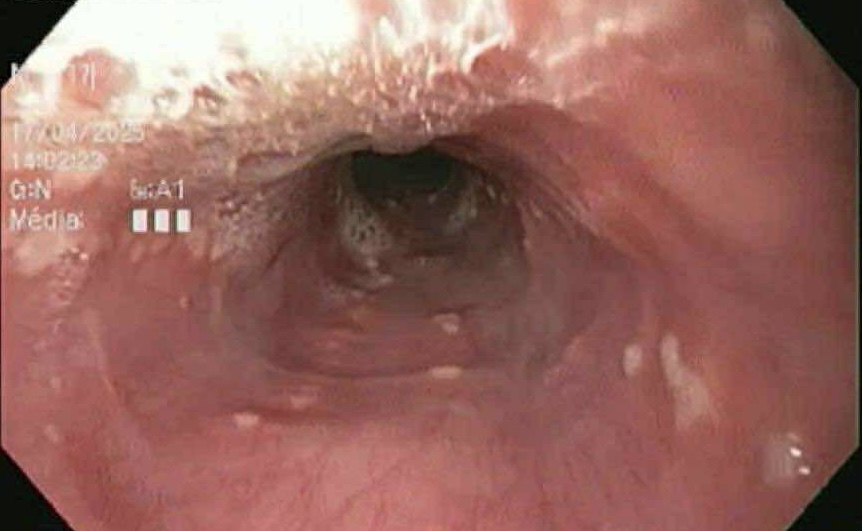
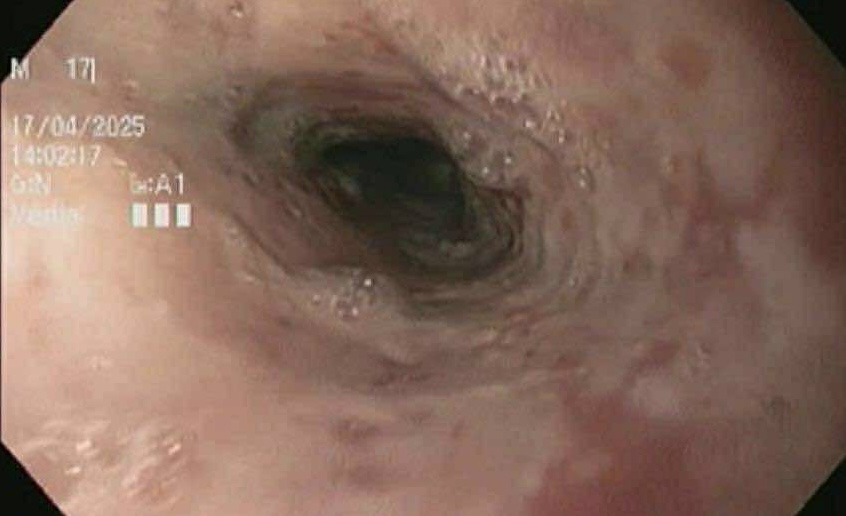
Upper endoscopy revealed esophageal ulcers, "bamboo-joint-like junctions' at the esophagus's middle and lower part, and partial duodenal bulb stenosis. The stomach was unremarkable. Ileo-colonoscopy showed no macroscopic findings. Biopsies were taken from ulcerated lesions in the esophagus. Histology revealed epithelial denudation, accompanied by diffuse, moderate to dense inflammatory infiltrates of lymphocytes, plasma cells, neutrophils, and numerous scattered macrophages. There was evidence of inflammatory granulation tissue with focal necrosis and one granuloma. Periodic acid–Schiff (PAS) staining showed no evidence of fungal elements, ruling out mycotic involvement. Proton pump inhibitors (PPI) and antifungals were administered initially. After the biopsy result, prednisolone and sucralfate were added, and the patient responded very well to corticosteroid therapy. Currently, the patient is on maintenance therapy with budesonide and PPI. Discussion: The diagnosis and treatment of esophageal CD is challenging. To our knowledge, we have not identified any reports of them in Albania. The workup to diagnose esophageal CD should include a clinical evaluation, baseline laboratory tests, endoscopic evaluation, histological assessment, and exclusion of other causes of esophagitis. Corticosteroids help manage acute inflammation; anti-tumor necrosis factor (anti-TNF) and immunomodulators remain the mainstay of therapy for esophageal Crohn's. In conclusion, clinicians should consider CD in atypical presentations of esophageal disease.
Figure: Esophageal ulcers
Figure: "Bamboo-joint-like junctions' at the esophagus.
Disclosures: Denisa Horanlli indicated no relevant financial relationships. Fjona Tabaku indicated no relevant financial relationships. Suela Ristollari indicated no relevant financial relationships. Aida Haxhillari indicated no relevant financial relationships. Qirjako Gjino indicated no relevant financial relationships.
Denisa Horanlli, MD1, Fjona Tabaku, MD, MPH2, Suela Ristollari, MD3, Aida Haxhillari, MD4, Qirjako Gjino, MD5. P5550 - When Crohn’s Climbs Higher: Esophageal Crohn's Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpeg.jpg "Denisa Horanlli, MD (she/her/hers) photo")