Chusila Lee, DO1, William M. LaShomb, MD1, Christina Awad, MD2 1Brooke Army Medical Center, San Antonio, TX; 2San Antonio Uniformed services Health Education Consortium, San Antonio, TX Introduction: Isolated duodenal Crohn’s disease (CD) is an uncommon phenotype accounting for less than 1% of all Crohn’s disease cases. Severe ulceration & bleeding in duodenal Crohn’s is uncommon & little is known about the efficacy of small molecule therapies as rescue agents in these cases. We present a case of successful Upadacitinib (UPA) rescue therapy in a patient with isolated duodenal CD & life-threatening hemorrhage.
Case Description/
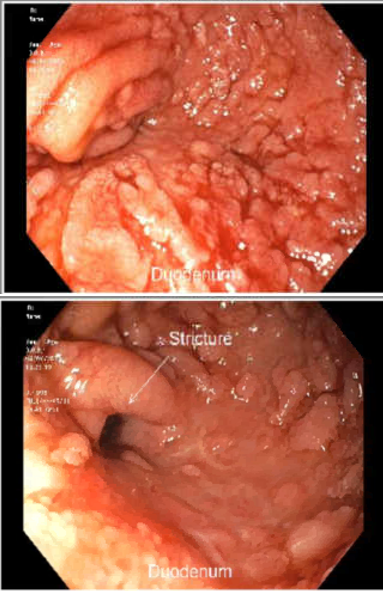
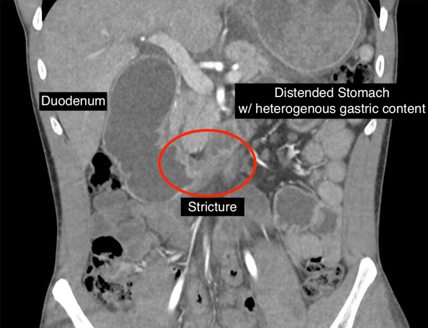
Methods: A 29-year-old male with 7 years of duodenal CD presented with abdominal pain & coffee-ground emesis. He was previously on infliximab (IFX) but had been lost to follow up. IFX antibodies were not detected suggesting loss of response was not due to antibody formation. CTA demonstrated gastric outlet obstruction (GOO) with duodenal stricture [1]. Initial EGD revealed cavernous dilation of the duodenal bulb & a distal stricture with oozing, friable mucosa [2]. As there was no specific bleeding target, no hemostatic therapy was used. Dilation was deferred given risk of perforation. Passage of an enteral feeding tube was attempted with an ultrathin endoscope, fluoroscopy & wire but ultimately failed. Biopsies confirmed Crohn’s without dysplasia or malignancy. Ileo-colonoscopy was normal.
IV corticosteroids were started, but bleeding persisted requiring 4 units of PRBC. Given a low albumin of 1.7g/dl and a concern for IFX loss of response, high dose (30mg BID) UPA was initiated as rescue therapy. Over multiple days, his transfusion requirement improved, and he was able to advance his diet to low residue, although on repeat upper endoscopy at ten days, a (now traversable) duodenal stricture persisted and was referred to surgery as an outpatient. He was transitioned to the standard UPA load prior to discharge. He has not required hospitalization for bleeding or outlet obstruction since. Discussion: Treatment of bleeding, stricturing duodenal CD presents many challenges. In our case, high dose corticosteroids were inadequate for rapid improvement of mucosal inflammation & bleeding. Loss of response with malnutrition & significant hypoalbuminemia made protein bound IFX a poor choice for rescue therapy. We chose to start high dose UPA (30mg BID), which is effective irrespective of albumin. While it is difficult to attribute the improvement solely to UPA, our patient was able to wean off steroids and remained free of additional hospitalization on monotherapy. He is being evaluated for surgical management for the stricture to include Whipple or duodenal stricturoplasty.
Figure: [1] CTA abdomen/pelvis demonstrating a gastric outlet obstruction with duodenal stricture
Figure: [2] EGD revealing cavernous dilation of the duodenal bulb & a distal stricture with oozing, friable mucosa
Disclosures: Chusila Lee indicated no relevant financial relationships. William LaShomb indicated no relevant financial relationships. Christina Awad indicated no relevant financial relationships.
Chusila Lee, DO1, William M. LaShomb, MD1, Christina Awad, MD2. P5527 - Upadacitinib Rescue Therapy for Bleeding Duodenal Crohn’s Disease: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")