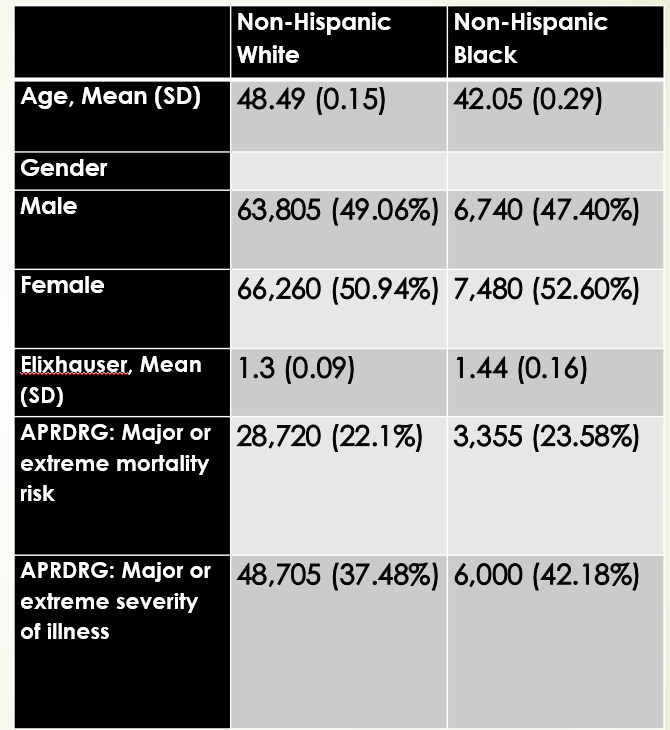
Priyata Dutta, MD1, Duresha D. Malik, MD2, Remonda Khalil-Moawad, MSPH3, Jane Wong, MPH, CCRP1, Chin-I Cheng, PhD4, Anupam Suneja, MBBS, MPH1 1Trinity Health Ann Arbor Hospital, Ypsilanti, MI; 2Ttinity Health Ann Arbor, Ypsilanti, MI; 3Trinity Health Ann Arbor Hospital, Ann Arbor, MI; 4Central Michigan University, Mt Pleasant, MI Introduction: Research shows significant disparities in morbidity, mortality, and length of stay (LOS) between Black and White patients undergoing surgery for inflammatory bowel disease (IBD). However, there is a lack of literature addressing how these racial inequities affect Failure to Rescue (FTR) in surgeries for IBD. Herein, we aim to address this gap by investigating the impact of patients race and ethnicity on FTR rates. Methods: In this retrospective cohort study, National Inpatient Sample (NIS) database was utilized to identify patients who had surgery for IBD between 2013 and 2019. FTR is the rate of death among patients who experience an adverse event and serves as a metric for surgical quality. The primary goal of our study was to assess FTR rates by race and ethnicity. Results: Between 2013 and 2019, a total of 159,470 patients underwent surgery for IBD, with majority being for Crohn’s disease (CD) (103,835). Most of these patients were White (81.56%). Black patients compared with White patients displayed higher Elixhauser comorbidity index (1.44 vs.1.3) and All Patient Refined DRG: Severity of index Subclass of major or extreme loss of function (42.18%vs.37.48%) (Table 1).
Black patients compared with White patients had a higher incidence of major adverse events (MAEs) (33.72% vs. 28.73%, P < 0.0001). At the same time, there was a significant trend of increasing MAEs among black patients (P< 0.001). Although black patients compared to white patients had higher percentages of FTR (2.18% vs. 2.19%) and inpatient mortality (2.22 vs. 2.12%), these were not significantly different.
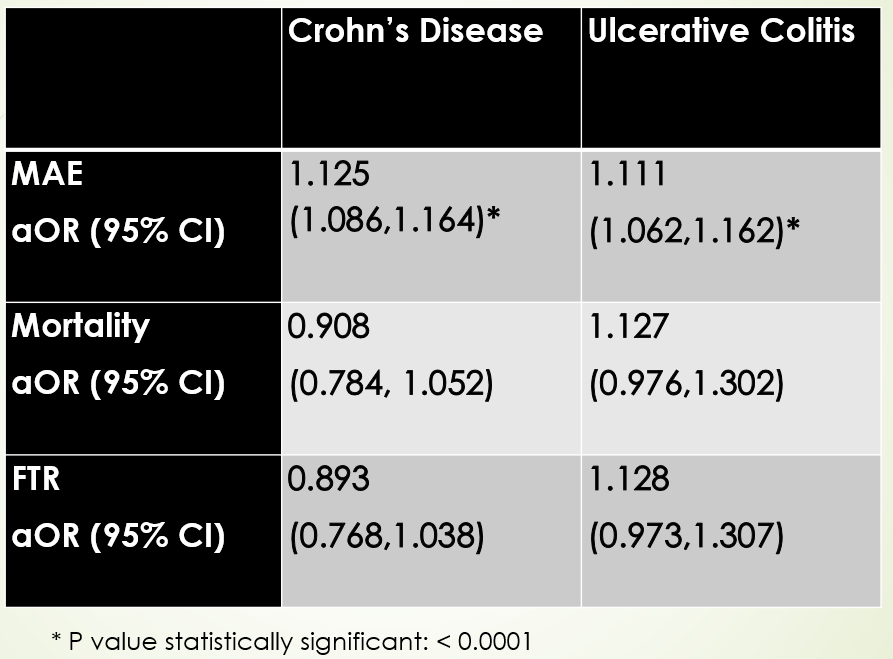
Multivariable logistic regression analysis showed Black patients with CD were more likely than White patients to experience FTR. However, these differences were not statistically significant. Similarly, Black patients with ulcerative colitis (UC) had lower rates of FTR and mortality rates (MR) with no statistically significant differences observed (Table 2). Discussion: Our analysis shows that Black patients undergoing surgery for IBD are more likely to experience major adverse events compared to White patients. However, there is no statistically significant difference in MR or FTR rates between the two groups. These findings suggest that clinicians are providing high-quality post-surgical care to Black patients, which helps prevent deaths despite the higher incidence of major adverse events. These findings support the view that race is a social construct rather than a biological determinant of FTR.
Figure: Table 1: Baseline characteristics of study population
Figure: Table 2: Study outcomes after multivariable logistic regression analysis MAE: Major Adverse Events; FTR: Failure to Rescues
Disclosures: Priyata Dutta indicated no relevant financial relationships. Duresha Malik indicated no relevant financial relationships. Remonda Khalil-Moawad indicated no relevant financial relationships. Jane Wong indicated no relevant financial relationships. Chin-I Cheng indicated no relevant financial relationships. Anupam Suneja indicated no relevant financial relationships.
Priyata Dutta, MD1, Duresha D. Malik, MD2, Remonda Khalil-Moawad, MSPH3, Jane Wong, MPH, CCRP1, Chin-I Cheng, PhD4, Anupam Suneja, MBBS, MPH1. P5476 - Impact of Racial Disparity on Failure to Rescue in Patients With Inflammatory Bowel Disease Undergoing Surgery: A NIS Database Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.