P5369 - Hospitalization Outcomes and Resource Utilization in Patients With Crohn’s Disease and Metabolic Syndrome: A National Inpatient Sample Analysis
Staten Island University Hospital, Northwell Health Staten Island, NY
Ryan Njeim, MD, Chapman Wei, MD, Elie Moussa, MD, Liliane Deeb, MD Staten Island University Hospital, Northwell Health, Staten Island, NY Introduction: A 2015 retrospective study found that patients with Crohn’s disease (CD) and metabolic syndrome (MetS) had double the rate of CD-related hospitalizations compared to CD patients without MetS. However, the effect of MetS on hospitalized CD patients has not been well studied. We aim to assess the effect of MetS in CD patients on their hospital-related outcomes. Methods: We conducted a retrospective cohort study using the NIS database 2016-2020. Using ICD-10 code, we identified patients with CD and metabolic factors (hypertension, diabetes, dyslipidemia, obesity). Assigning 1 point for each comorbidity, a combined metabolic score (CMS) >2 was diagnostic for MetS. We checked hospital mortality, length of stay, vasopressor use, intubation, central line insertion, number of any procedure and discharge disposition. Univariate and multivariate analysis were conducted using SAS 9.4. Results: Among 153, 255 CD patients, 2.46% had MetS. MetS patients were significantly more female (62.5% vs 56.6%), white (81% vs 78%) and covered by Medicare (57.4% vs 32.3%). Significant differences in census divisions, urban-rural locations, income ZIP codes were seen, with non-MetS patients located more in urban areas and having a higher economic status. MetS patients had a higher rate of critical care interventions such as intubation (3.7% vs 2.1%) and central line use (1.3% vs 0.9%) while being less likely to be discharged home (59.3% vs 74.5%). All p values were < 0.001.
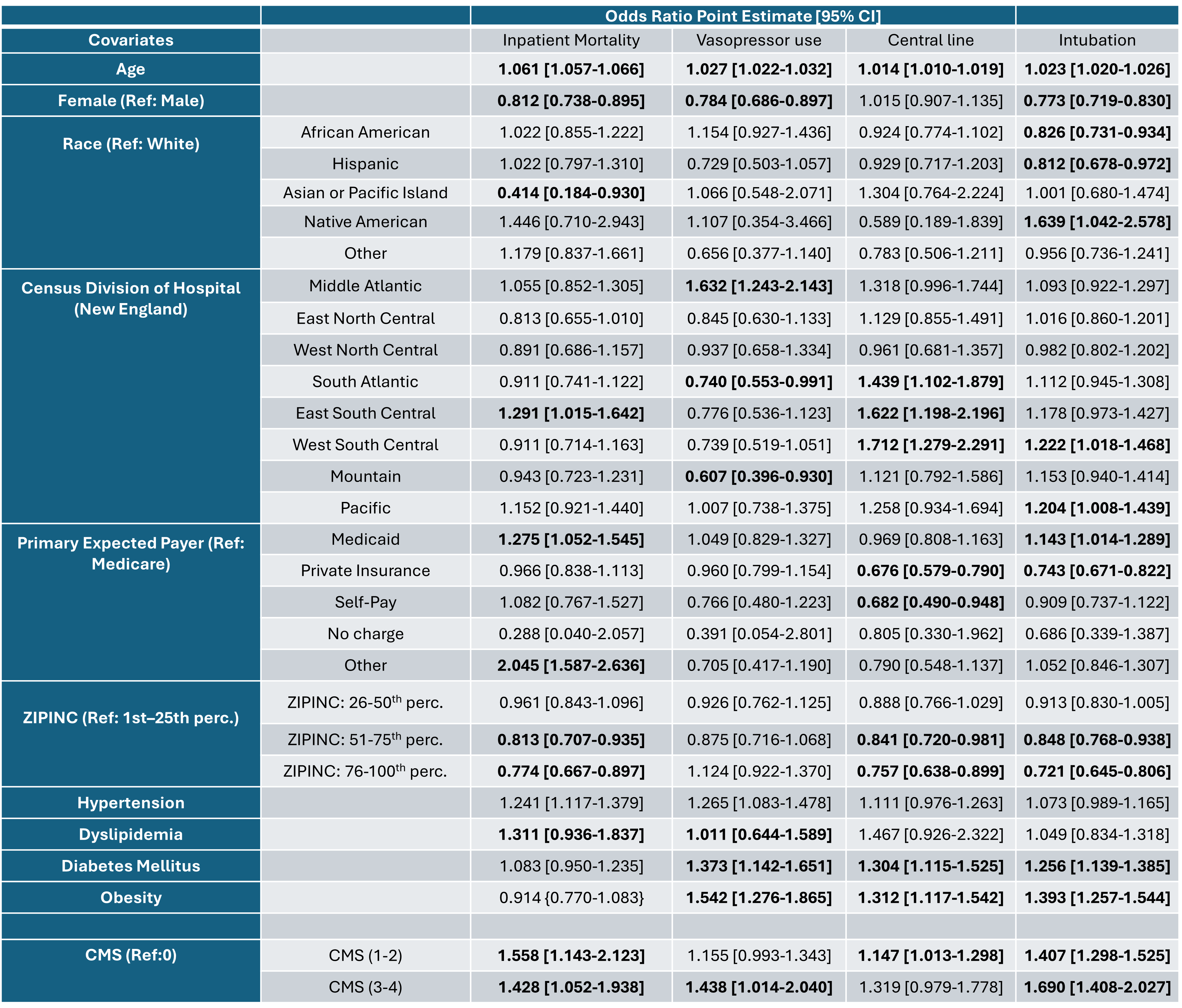
The multivariable analysis for inpatient mortality, central line use, vasopressor use and intubation are detailed in Table 1. Age was associated with higher odds of all 4 outcomes while higher income (ZIPINC 76–100%) was linked to lower odds (excluding vasopressor use). Regarding metabolic factors, hypertension, CMS 1-2 and CMS 3-4 were associated with higher mortality (OR 1.24, 1.56 and 1.43, respectively) while dyslipidemia was not associated with any of the outcomes. Obesity and diabetes were associated with higher odds of critical care interventions. Discussion: The presence of MetS in CD patients increased in-hospital morbidity and mortality leading to a more complicated hospital course and worse disposition on discharge. This study emphasizes the need for a targeted risk stratification and personalized treatment plan in CD patients with MetS. Further studies are needed to clarify the effect of strict management of MetS in this context on potential refinement of hospitalization outcomes.
Figure: Table 1: Association between hospital outcomes and metabolic factors in patients with Crohn's disease, adjusted for sociodemographic factors.
Disclosures: Ryan Njeim indicated no relevant financial relationships. Chapman Wei indicated no relevant financial relationships. Elie Moussa indicated no relevant financial relationships. Liliane Deeb indicated no relevant financial relationships.
Ryan Njeim, MD, Chapman Wei, MD, Elie Moussa, MD, Liliane Deeb, MD. P5369 - Hospitalization Outcomes and Resource Utilization in Patients With Crohn’s Disease and Metabolic Syndrome: A National Inpatient Sample Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")