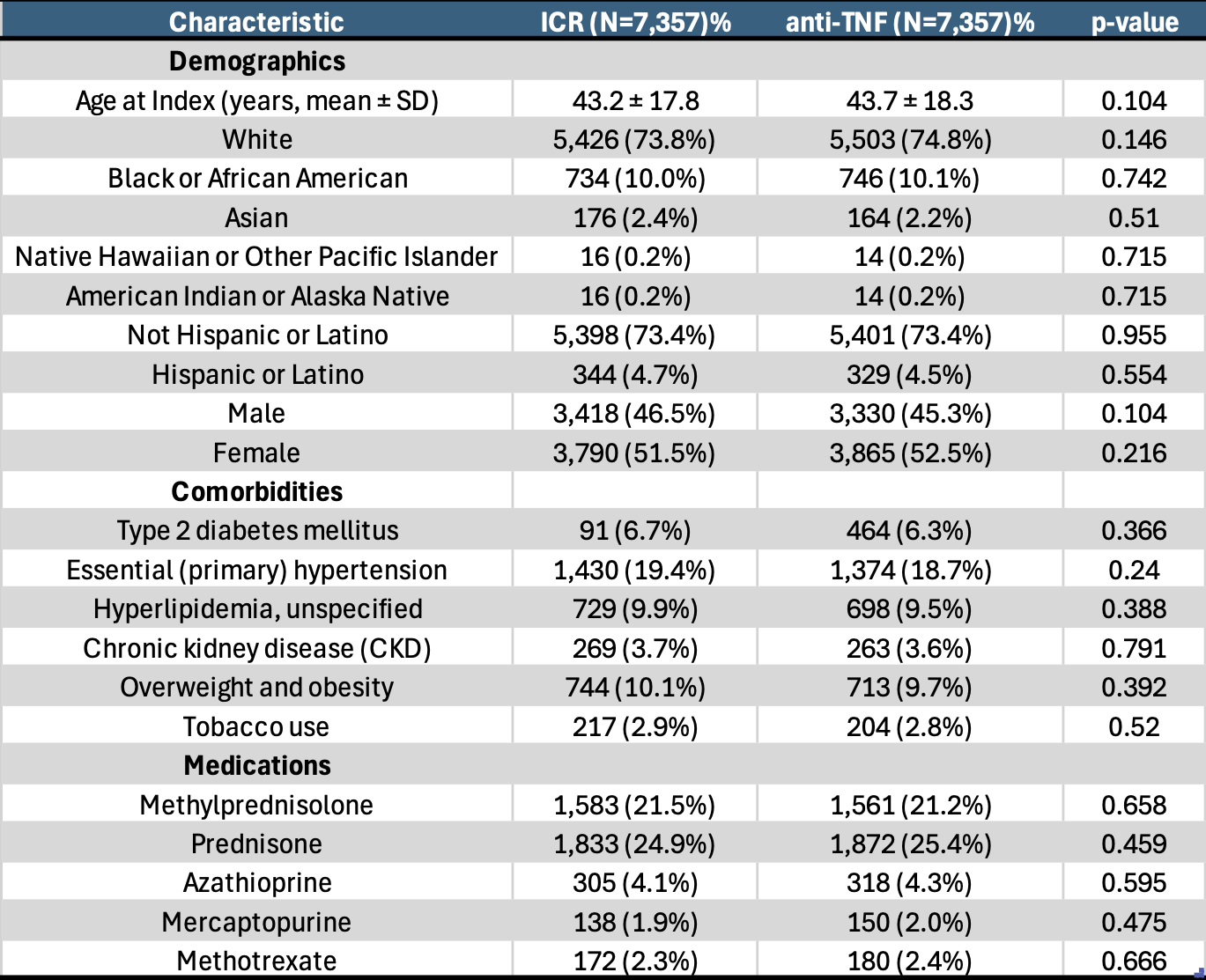
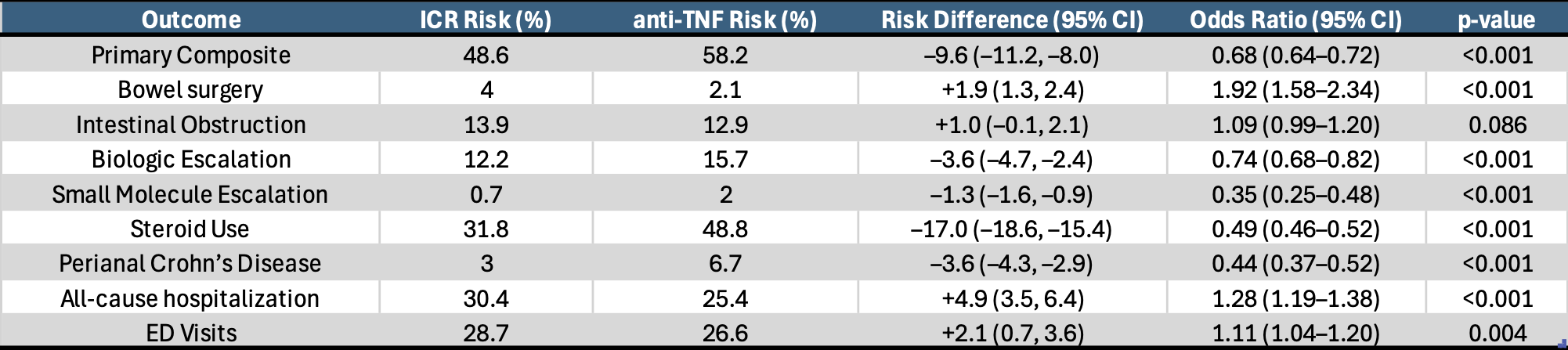
Mohamed Nadeem, MD1, Prabhat Kumar, MD2, Archana Kharel, MD3, Basil Jalamneh, MD4, Taha Qazi, MD4 1Cleveland Clinic Foundation, Fairview Park, OH; 2Virginia Commonwealth University, Richmond, VA; 3Cleveland Clinic, Cleveland, OH; 4Cleveland Clinic Foundation, Cleveland, OH Introduction: Anti-tumor necrosis factor (TNF) therapy remains integral for the management of Crohn’s disease (CD). However, recent evidence, such as the Laparoscopic Ileocolonic Resection Versus Infliximab Treatment of Recurrent Distal Ileitis in Crohn’s Disease trial, shows that early surgical intervention, particularly ileocolonic resection (ICR), may provide similar or even superior outcomes, along with decreased long-term dependence on pharmacologic therapy. This study evaluated long-term clinical outcomes among CD patients treated with early ICR versus early initiation of anti-TNF therapy within one year of diagnosis. Methods: A retrospective, propensity score-matched cohort study was conducted using TriNetX Global Collaborative Network. We compared 7,357 patients undergoing early ICR with an equal number of patients initiating anti-TNF therapy within one year of CD diagnosis. Matching controlled for demographics, comorbidities, and baseline medication use. The primary composite outcome included all-cause hospitalization, steroid use, escalation of Crohn’s therapy, and bowel surgery. Secondary outcomes individual components of primary outcomes, perianal disease, intestinal obstruction, and emergency department (ED) visits. Outcomes were evaluated over a 10-year follow-up period. Risks, risk differences, odds ratios (ORs), and 95% confidence intervals (CIs) were reported. Results: The ICR group showed a significantly lower risk of the primary composite outcome (48.6% vs. 58.2%; OR 0.68, CI 0.64–0.72; p< 0.001). ICR was also associated with reduced risk of biologic escalation (12.2% vs. 15.7%; OR 0.74; p< 0.001), small molecule escalation (0.7% vs. 2.0%; OR 0.35; p< 0.001), steroid use (31.8% vs. 48.8%; OR 0.49; p< 0.001), and perianal disease (3.0% vs. 6.7%; OR 0.44; p< 0.001). However, ICR was associated with higher rates of bowel surgery (4.0% vs. 2.1%; OR 1.92; p< 0.001), all-cause hospitalization (30.4% vs. 25.4%; OR 1.28; p< 0.001), and ED visits (28.7% vs. 26.6%; OR 1.11; p=0.004). No statistically significant difference was observed in the development of intestinal obstruction (13.9% vs. 12.9%; p</em>=0.086). Discussion: Among Crohn’s disease patients, early ICR is associated with significantly reduced long-term corticosteroid use, therapy escalation, and perianal complications compared to early anti-TNF therapy. While it carries a higher risk of repeat surgery and hospitalizations, these findings support early surgical resection as a viable therapeutic option in selected patients.
Figure: Table 1: Matched baseline characteristics of Ileoclonic resection cohort and anti-tumor necrosis factor therapy cohort with Crohn's disease
Figure: Table 2: Clinical outcomes at 10 year follow up comparing early ileocolinc resection versus anti-tumor necrosis factor therapy in Crohn's Disease.
Disclosures: Mohamed Nadeem indicated no relevant financial relationships. Prabhat Kumar indicated no relevant financial relationships. Archana Kharel indicated no relevant financial relationships. Basil Jalamneh indicated no relevant financial relationships. Taha Qazi: Abbvie – Advisor or Review Panel Member, Advisory Committee/Board Member, Consultant, Grant/Research Support, Speakers Bureau. Celltirion – Grant/Research Support. Eli Lilly – Advisor or Review Panel Member, Advisory Committee/Board Member, Consultant. Johnson and Johnson – Advisor or Review Panel Member, Advisory Committee/Board Member, Consultant, Speakers Bureau. pfizer – Grant/Research Support.
Mohamed Nadeem, MD1, Prabhat Kumar, MD2, Archana Kharel, MD3, Basil Jalamneh, MD4, Taha Qazi, MD4. P5329 - Long-Term Comparative Outcomes of Early Ileocolic Resection versus Anti-TNF Therapy in Crohn’s Disease Patients, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.