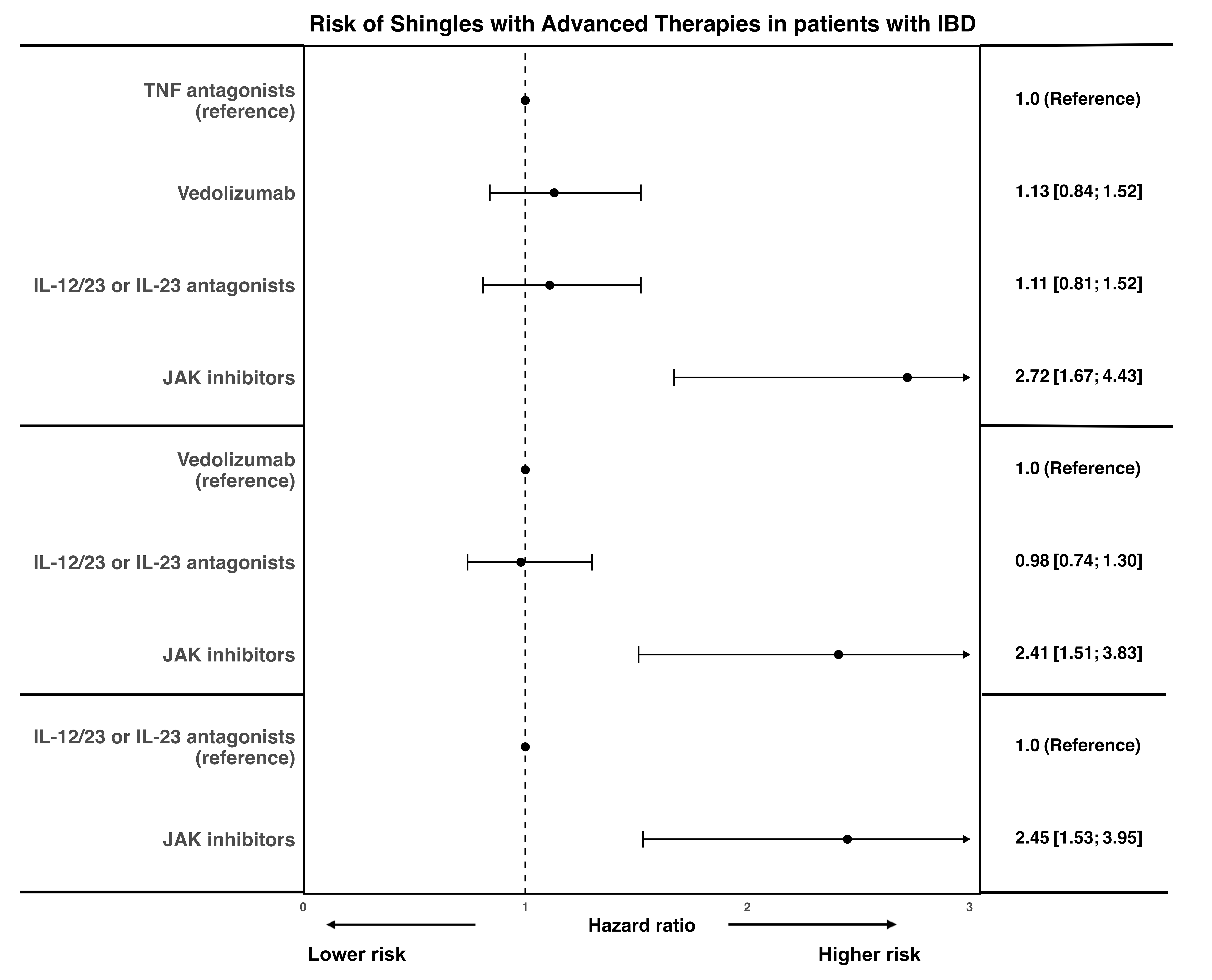
Dhruv Ahuja, MBBS1, Soo-Kyung Park, MD, PhD2, Kuan-Hung Yeh, 3, Sagar Patel, BS2, Shane Goodwin, PhD4, Christopher Ma, MD, MPH5, Namrata Singh, MD6, Ashwin Ananthakrishnan, 7, Vipul Jairath, MBChB, DPhil, MRCP8, Ronghui Xu, PhD2, Siddharth Singh, MD, MS2 1University of California San Diego, Delhi, Delhi, India; 2University of California San Diego, San Diego, CA; 3University of California San Diego, La Jolla, CA; 4Western University, London, ON, Canada; 5University of Calgary, Calgary, AB, Canada; 6University of Washington, Seattle, WA; 7Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, Boston, MA; 8Department of Medicine and Department of Epidemiology and Biostatistics, Western University, London, ON, Canada Introduction: We conducted a retrospective cohort study comparing the risk of shingles with advanced therapies in patients with Inflammatory bowel disease (IBD) Methods: Using an administrative claims database, we identified patients with IBD who initiated treatment with either tumor necrosis factor-α (TNF) antagonists (infliximab, adalimumab, golimumab and certolizumab pegol), anti-integrin agents (vedolizumab), anti-interleukin (IL)-12/23p40 or anti-IL-23p19 agents (ustekinumab, risankizumab, mirikizumab, collectively labeled anti-interleukins), or Janus kinase (JAK) inhibitors (tofacitinib, upadacitinib) between 2016 and 2023, and had insurance coverage for at least 1y before and after treatment initiation. We assessed the incidence rate (IR per 100 person-year [PY]) of shingles (overall and complicated, including post herpetic neuralgia ocular and neurologic involvement) and compared risks using inverse probability of treatment weighting (IPTW). Propensity scores were estimated through generalized boosted models incorporating demographics, comorbidities, healthcare utilization, and prior/concomitant IBD therapies. Weighted Cox models estimated hazard ratios (HR) and 95% confidence intervals (CI). Results: We included 21,564 patients with IBD (mean age range, 45-49 years; 51-53% females; 6% with zoster vaccination) followed over 27 months. The incidence of shingles and complicated shingles varied with difference advanced therapies: TNF antagonists (n=9,385; IR of shingles/complicated shingles per 100-py, 1.00/0.30), anti-integrin agents (n=5,881; IR, 1.38/0.43), anti-interleukins (n=5,445; IR, 1.24/0.45) and JAK inhibitors (n=853; IR, 3.33/0.88). After adjusting for confounding variables using IPTW, JAK inhibitors were associated with higher risks of shingles compared with TNF antagonists (HR, 2.72 [95% CI, 1.67-4.43]), anti-integrin agents (HR, 2.41 [1.51-3.84]) and anti-IL 12/23p40 agents or anti-IL-23p19 (HR, 2.45 [1.53-3.95]). Similar trends were observed for risk of complicated shingles. No differences were observed in the risk of shingles between TNF antagonists, anti-integrins and anti-interleukins (Figure 1). Discussion: In this large real-world cohort of patients with IBD, JAK inhibitors were associated with higher risks of overall shingles compared to other advanced therapies. No differences were observed in the risk of shingles with other advanced therapies, with overall incidence ranging from 1.0-1.4 per 100-py.
Figure: Figure 1. Comparative risk of shingles with advanced therapies in patients with IBD