Ana Finke Abbott, MD, Triston Berger, MD, Reid Hopkins, MD, Naveen Anand, MD Norwalk Hospital, Norwalk, CT Introduction: Upper gastrointestinal (GI) bleeding is defined as bleeding originating proximal to the ligament of Treitz. It typically manifests as hematemesis or melena with anemia. Isolating the source of bleeding is not always straightforward, and a thorough understanding of anatomy with careful diagnostic evaluation is required. We present a case of upper GI bleeding secondary to a splenic artery pseudoaneurysm with retroperitoneal hemorrhage draining into the stomach via a spontaneous cystogastrostomy.
Case Description/
Methods: A 54-year-old male with a history of alcohol use disorder, chronic calcified pancreatitis, and stage IV pancreatic adenocarcinoma presented for abdominal pain. One month earlier, endoscopic ultrasound (EUS) with biopsies was done for a pancreatic mass, which confirmed adenocarcinoma. Sonographic findings included invasion into the superior mesenteric artery, but a preserved interface of the celiac trunk and portal vein, suggesting no direct invasion.
One month later, he returned to the ED with acute abdominal pain, melena, and a significant drop in hemoglobin. CT abdomen showed resolution of a previously seen pancreatic tail pseudocyst. Esophagogastroduodenoscopy (EGD) revealed no obvious source of bleeding. A spontaneous cystogastrostomy with purulent drainage into the stomach was identified, suggesting fistulization of the pseudocyst. The following day, the patient developed hematemesis and a further drop in hemoglobin. CT angiography revealed a 1.9 cm splenic artery pseudoaneurysm with surrounding retroperitoneal hemorrhage, and a defect in the posterior stomach wall connecting to the retroperitoneal fluid. This constellation of findings suggested that the presentation of GI bleeding was from a retroperitoneal bleed tracking into the stomach via the fistula formed by spontaneous cystogastrostomy. The patient underwent successful embolization of the pseudoaneurysm by interventional radiology. Follow-up CT showed >50% splenic infarction. Hemoglobin remained stable over 48 hours, and the patient was discharged. Discussion: This case highlights a unique cause of upper GI bleeding due to a retroperitoneal bleed from a splenic artery pseudoaneurysm with subsequent drainage into the stomach from a spontaneous cystogastrostomy tract. It demonstrates the importance of maintaining a broad differential in patients with GI bleeding and complex pathology, where early diagnosis can be lifesaving.
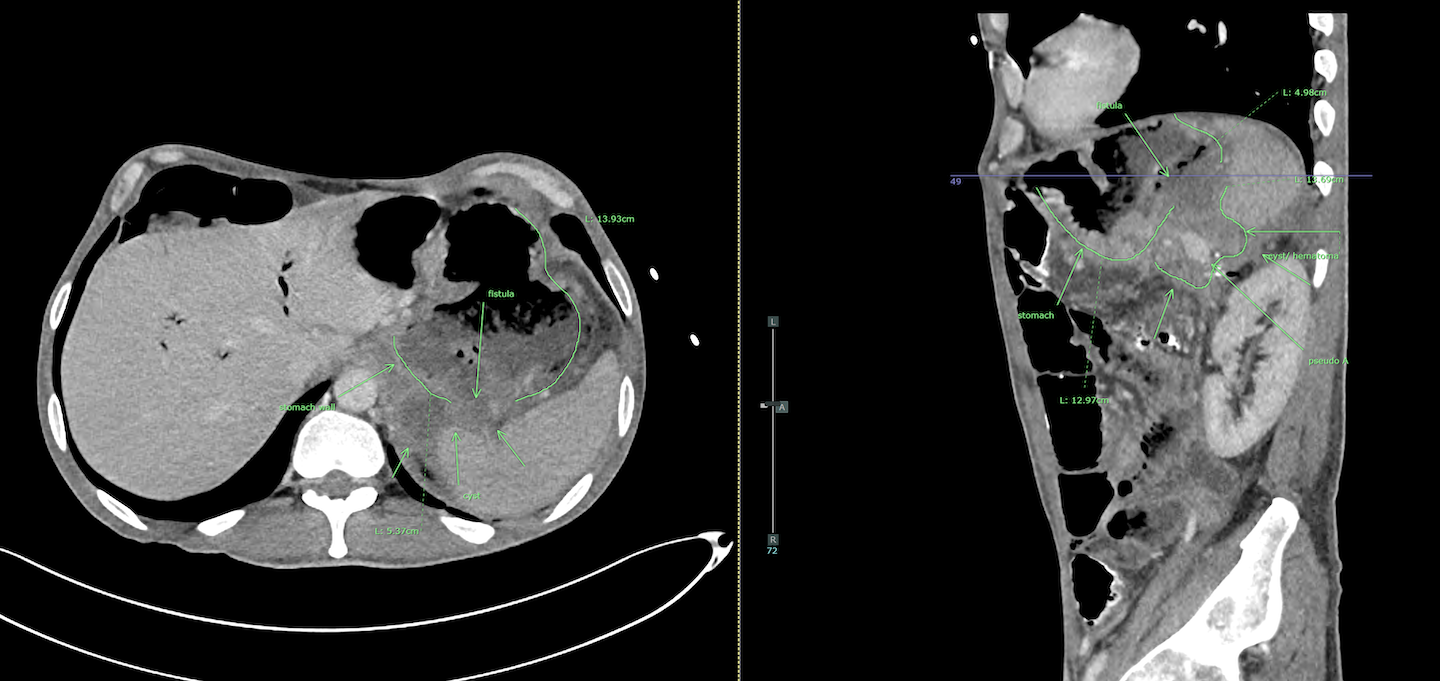
Figure: spontaneous cystogastrostomy with purulent drainage into the stomach
Figure: retroperitoneal bleed tracking into the stomach via the fistula formed by spontaneous cystogastrostomy
Disclosures: Ana Finke Abbott indicated no relevant financial relationships. Triston Berger indicated no relevant financial relationships. Reid Hopkins indicated no relevant financial relationships. Naveen Anand indicated no relevant financial relationships.
Ana Finke Abbott, MD, Triston Berger, MD, Reid Hopkins, MD, Naveen Anand, MD. P5296 - The Path Less Traveled: GI Bleed Secondary to Retroperitoneal Pseudoaneurysm Rupture, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.