Rida Aziz, DO1, Lauren Morrison, MD2, Katherine DiPastina, DO3 1Inspira Health Network, Glassboro, NJ; 2Inspira Health, Glassboro, NJ; 3Inspira Health, Mullica Hill, NJ Introduction: A Dieulafoy's lesion (DL) is a rare cause of gastrointestinal (GI) bleed in which a a large 1-3mm tortuous submucosal artery erodes through the covering epithelium without associated mucosal ulceration. These uncommon causes of GI bleeding mostly occur in the lesser curvature of the stomach from branches of the left gastric artery and are associated with mortality rates as high as 80%. Initial EGDs may be negative in up to 30% of cases due to size and location.
Case Description/
Methods: A 64-year-old female with atrial fibrillation, mechanical mitral valve on warfarin, and chronic kidney disease presented for 1 day of hematemesis and melena. Imaging was negative for active extravasation of contrast. Laboratory testing revealed a supratherapeutic INR of 5.5 and a hemoglobin of 6.1 with inadequate response to 2 units packed red blood cells (pRBC). Initial esophagogastroduodenoscopy (EGD) revealed grade B esophagitis and no obvious source of bleeding. However, the patient continued to show clinical signs of acute blood loss with persistent episodes of hematemesis, melena and anemia necessitating a total of 6 units pRBCs, 3 fresh frozen plasma and vitamin K. Repeat EGD revealed actively bleeding lesion of proximal jejunum. Hemostasis was achieved with 3 clips, BICAP cautery and tattoo injection. The patient was started on heparin before being transitioned back to warfarin without further GI bleeding. Discussion: Our case highlights a rare but serious cause of GI bleed. DLs are vascular malformations of the GI system that can cause profuse blood loss. Although the mechanism of action remains widely debated, the most accepted theory is that they form from the erosion of arteries in the stomach lining because of age-related atrophy or caustic agents such as alcohol and aspirin. DLs account for only 1-2% of GI bleeds. While endoscopy remains the gold standard for diagnosis and treatment, initial EGDs can be negative in 30% of cases. Thus initial EGD negative for DLs does not rule out the condition and a high index of suspicion is required for these lesions.
Figure: Actively bleeding small bowel lesion
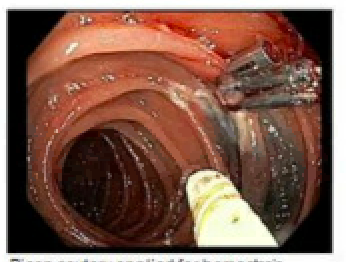
Figure: Hemostasis achieved after 3 endoclips and BiCAP cautery
Disclosures: Rida Aziz indicated no relevant financial relationships. Lauren Morrison indicated no relevant financial relationships. Katherine DiPastina indicated no relevant financial relationships.
Rida Aziz, DO1, Lauren Morrison, MD2, Katherine DiPastina, DO3. P5292 - A Rare Case of Acute Bleed of a Jejunal Dieulafoy’s Lesion With a Negative Initial EGD, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.