Mohamed A. Ebrahim, MD1, Yasmin Gerais, MBBS, MD2, Muhammad Sohaib Alvi, MBBS, MD1, Fares Hamad, DO3, Sammy Hamad, DO4, Laura Hamad, DO4, Bachar Hamad, MD4 1Ascension Saint Joseph Hospital, Chicago, IL; 2Saint Joseph medical center, Plainfield, IL; 3Ascension Saint Joseph Hospital, Joliet, IL; 4St. Joseph's Medical Centre, Joliet, IL Introduction: Gastric metastases from renal cell carcinoma (RCC) are exceedingly rare in clinical practice, with reported occurrences in only approximately 0.2% of RCC cases [1]. We report a case of upper GI bleeding from a peptic ulcer that histologically revealed metastatic clear cell RCC.
Case Description/
Methods: A 61-year-old male with a past medical history significant for DM, CKD, RCC treated with nephrectomy 26 years ago, and a known history of PUD, presented to the emergency department with vomiting and three episodes of hematemesis. He denied alcohol use, steroid intake, or significant NSAID use, and was not on anticoagulation, aside from daily low-dose aspirin. He had a previous hospitalization in 2023 for hematemesis, treated conservatively. On examination, the patient was hemodynamically stable. Laboratory investigations revealed a hemoglobin of 11.6 g/dL and a microcytic anemia with MCV of 73 fL. An esophagogastroduodenoscopy (EGD) showed oozing gastric ulcers and a Dieulafoy lesion, as shown in Figure 1. Hemostasis was achieved with injection therapy and argon plasma coagulation (APC). Biopsies were taken from the ulcer site. Histopathologic examination of the gastric ulcer biopsy revealed ulcerated and inflamed gastric mucosa containing metastatic clear cell renal cell carcinoma, as shown in Figure 2. Immunohistochemical staining confirmed the diagnosis, showing tumor cell positive for cytokeratin AE1/AE3, PAX-8, and Ki-67 with 9% nuclear positivity, while staining was negative for CK7, CK20, CDX2, CD45, and p53. Discussion: Patients with gastric metastases from RCC often exhibit widespread disease, and overall prognosis remains poor. Although the survival benefit of surgical resection for gastric metastases is not well established, localized resection may be considered in selected cases, particularly when bleeding is present and no other metastatic disease is identified. Previous literature has identified certain factors associated with worse outcomes in RCC patients with gastric metastases, including a grossly protruding gastric lesion, presence of additional metastatic sites, and a short interval, less than 6.3 years, between initial RCC treatment and diagnosis of gastric spread [2]. In our case, a protruding gastric lesion was discovered just 28 years after RCC diagnosis, aligning with previously described high-risk features and underscoring the aggressive nature of disease progression. Immunohistochemical markers like PAX-8 are crucial in identifying renal origin in metastatic tumors.
Figure: Oozing gastric ulcer with an exposed vessel, consistent with a Dieulafoy lesion. The ulcer appears irregular with heaped-up margins and a central depression.
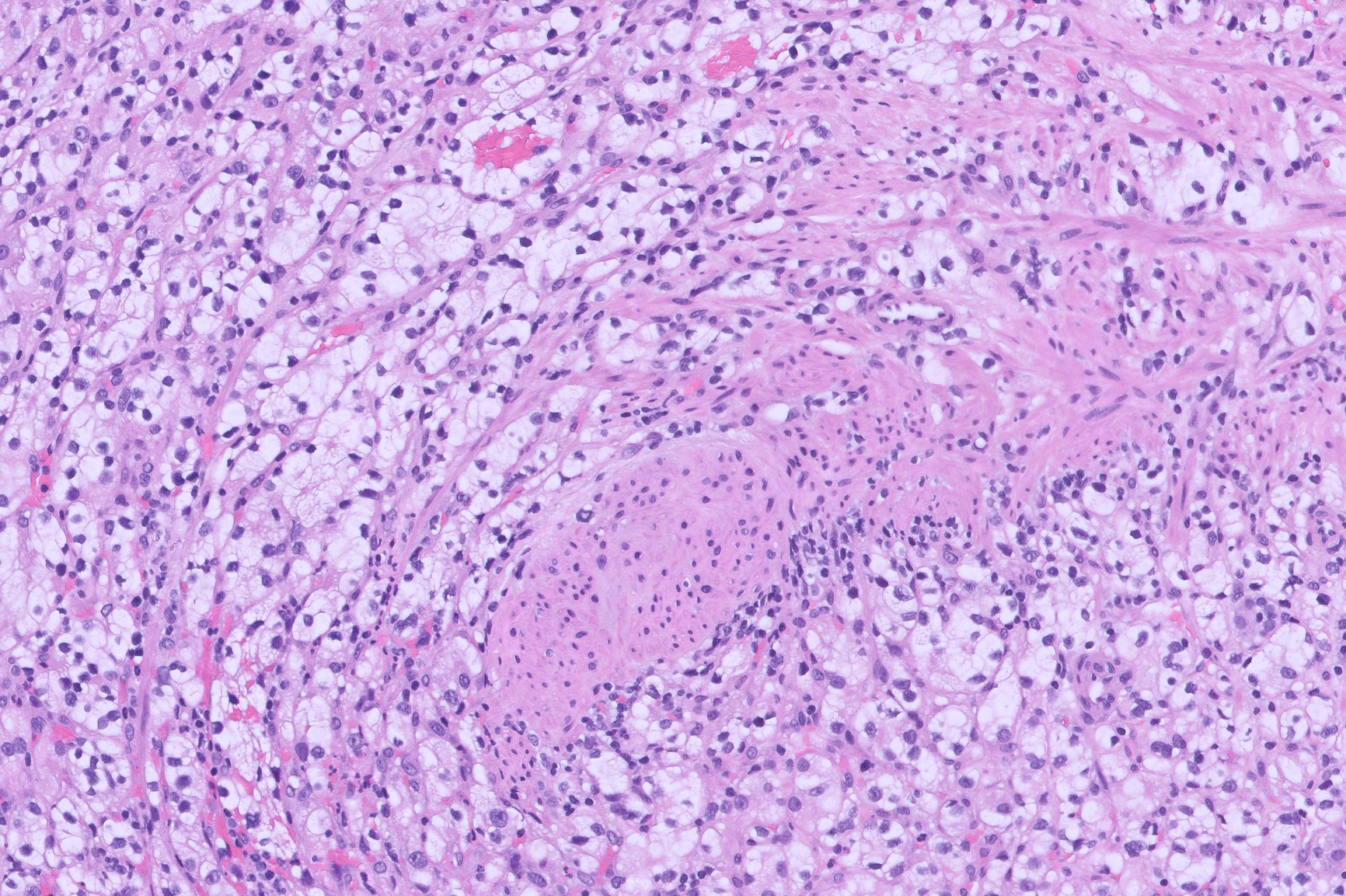
Figure: Ulcerated and inflamed gastric mucosa representing clear cell renal cell carcinom, suggestive of metastatic RCC
Disclosures: Mohamed Ebrahim indicated no relevant financial relationships. Yasmin Gerais indicated no relevant financial relationships. Muhammad Sohaib Alvi indicated no relevant financial relationships. Fares Hamad indicated no relevant financial relationships. Sammy Hamad indicated no relevant financial relationships. Laura Hamad indicated no relevant financial relationships. Bachar Hamad indicated no relevant financial relationships.
Mohamed A. Ebrahim, MD1, Yasmin Gerais, MBBS, MD2, Muhammad Sohaib Alvi, MBBS, MD1, Fares Hamad, DO3, Sammy Hamad, DO4, Laura Hamad, DO4, Bachar Hamad, MD4. P5238 - Unveiling a Renal Intruder Behind GI Bleeding: A Clear Cell Surprise in the Stomach 26 Years After Nephrectomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")