Azeem Khalid, MD1, Asad Ur Rehman, MD2, Muhammad Ahsan Asif, MBBS3, Muhammad Raffey Shabbir, MD4, Ibrar Atiq, MD5 1Aiken Regional Medical Centers, Aiken, SC; 2Yale New Haven Hospital, New Haven, CT; 3Jinnah Hospital Lahore, Lahore, Punjab, Pakistan; 4Marshfield Medical Center, Marshfield, WI; 5United Health Services, Wilson Medical Center, Binghamton, NY Introduction: Hepatic artery aneurysms (HAAs) represent approximately 20% of all visceral aneurysms. Common causes include trauma, atherosclerosis, and medial degeneration. The majority of patients are asymptomatic before rupture and rupture is the first clinical manifestation in most cases. Rarely, upper gastrointestinal bleeding (UGIB) results from fistula formation between the hepatic artery and duodenum.
Case Description/
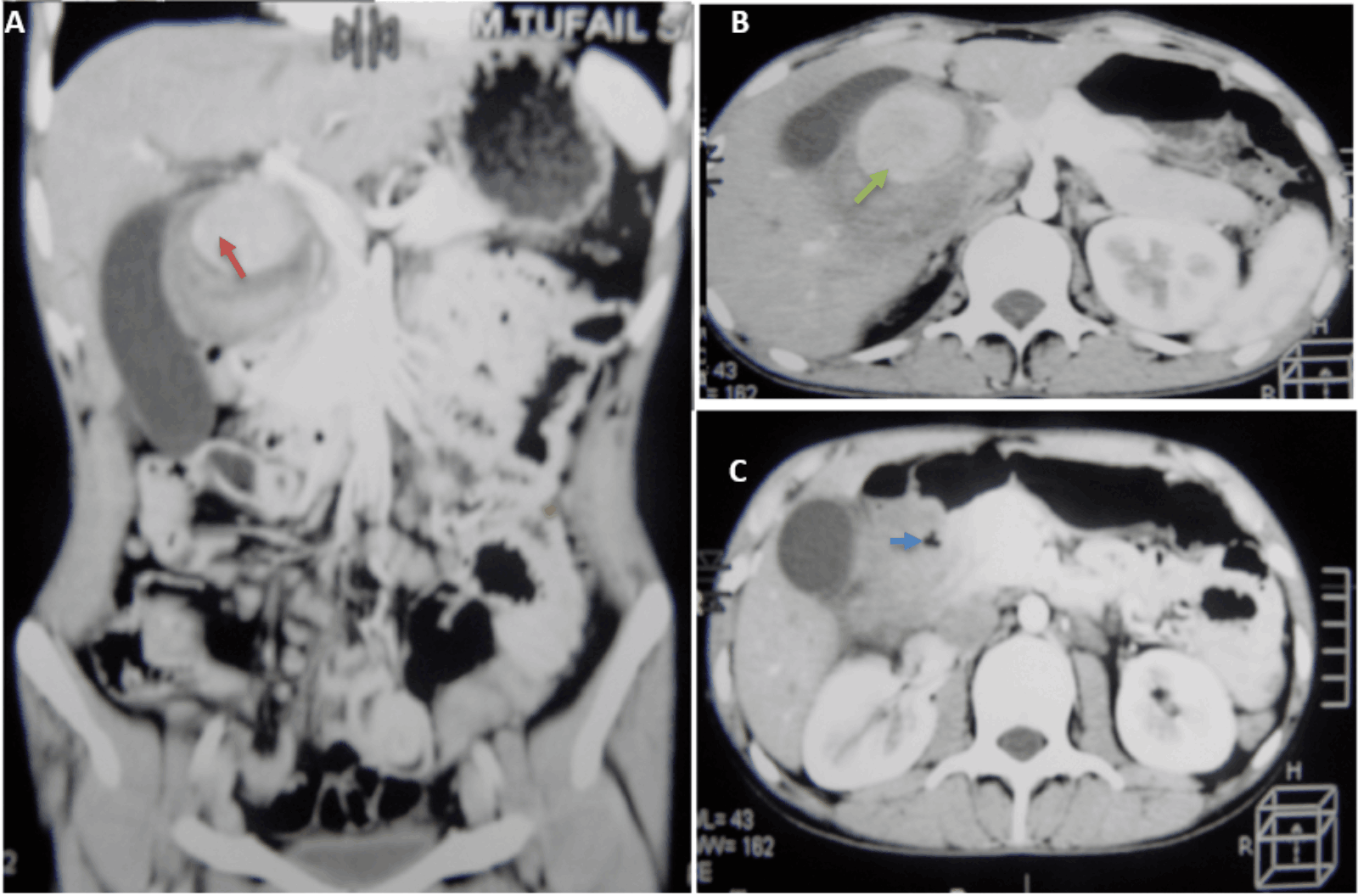
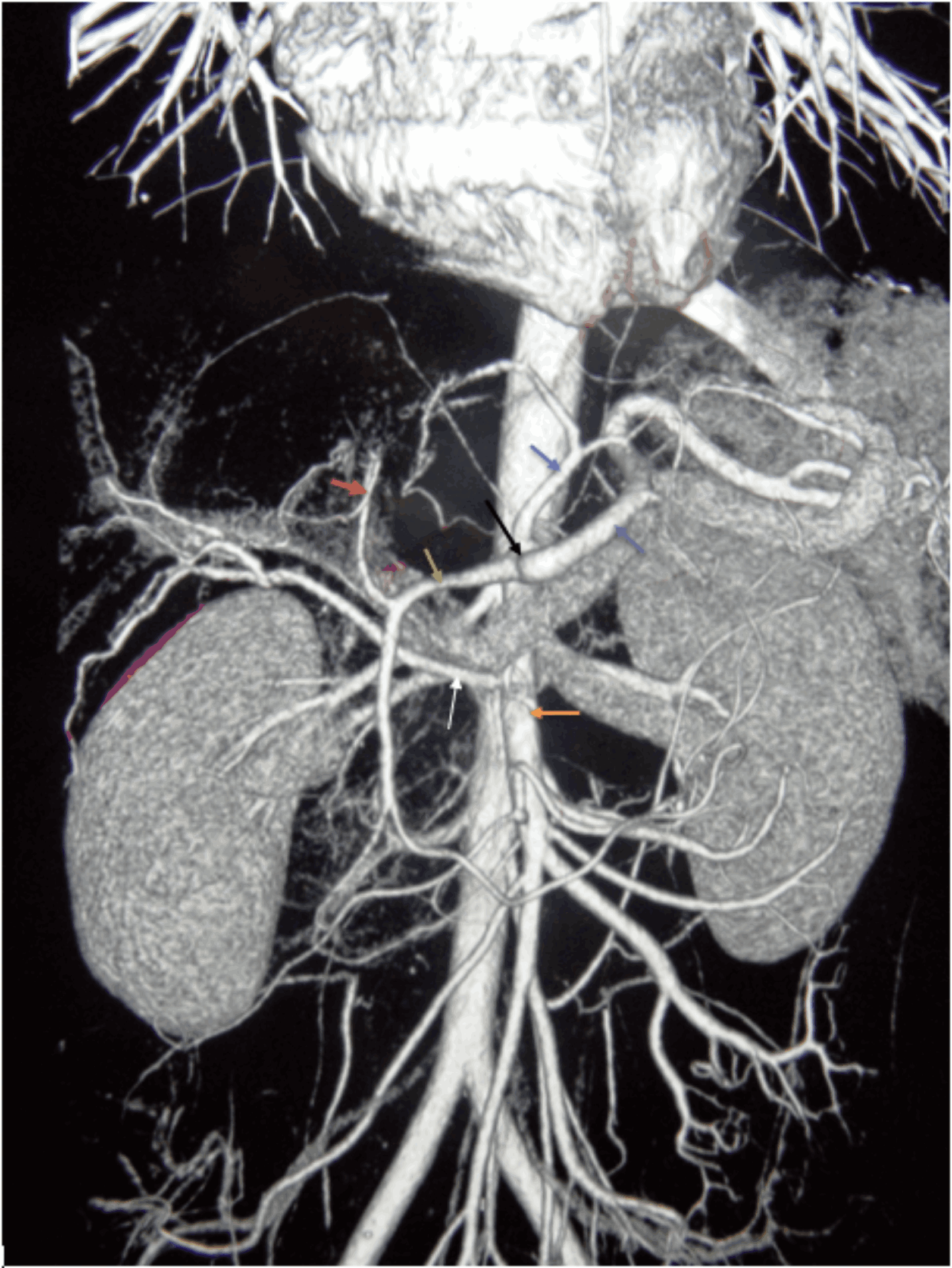
Methods: A 20-year-old male with a history of blunt abdominal trauma three years ago was admitted to the medical ward with complaints of right upper quadrant abdominal pain, melena, and hematemesis. Physical exam was remarkable for pallor and tachycardia except for anemia (hemoglobin: 6.6 g/dl), laboratory findings were unremarkable, including liver function tests (LFTs). Hepatitis and human immunodeficiency virus (HIV) screening were negative. Abdominal ultrasound revealed a pulsatile mass of 58 mm in diameter in the porta hepatis, and colour doppler showed bidirectional flow. A contrast-enhanced computed tomogram (CT) of the abdomen showed a 90 mm × 50 mm mass in the porta hepatis signifying hepatic artery pseudoaneurysm (HAP), and tiny air density foci were noted in the pseudoaneurysm signifying aneurysm-duodenal fistula (figure 1). A CT Angiogram revealed an accessory hepatic artery arising from the proximal superior mesenteric artery as a feeding artery (figure 2). An Upper GI endoscopy revealed a torrential amount of bile flowing from the ampulla of Vater, and an indentation was visualized on the medial wall of the second part of the duodenum. Patient underwent laparoscopic clipping of the feeding artery, and postoperative doppler studies confirmed the reduction in the size of the aneurysm as well as the absence of pulsatile flow through the aneurysm. The postoperative course was uneventful, and at one-year follow-up, the patient was asymptomatic. Discussion: HAAs, though rare, are a recognized cause of UGIB, accounting for 0.4% of cases, 20% of which are pseudoaneurysms. With a rupture risk of 21 to 80% and an associated mortality of 21 to 43%, early intervention is critical. HAPs can form fistulas with the duodenum, leading to UGIB. Definitive treatment depends upon the surgical ligation and aneurysmectomy with bypass grafting or with end-to-end anastomosis. In our patient, given the pseudoaneurysm’s size, robust hepatic collateral supply, and the patient’s low surgical risk, surgical ligation was performed.
Figure: Figure 1: Computed Tomogram of Abdomen with IV Contrast. A. Left panel is a coronal section through the abdomen showing a large mixed density mass with a whorled pattern in the porta hepatis indenting the neck of the gallbladder (red arrow). B. Right upper panel is an axial section through the abdomen showing a mixed-density pseudoaneurysm (green arrow). C. Right lower panel is also an axial section through the abdomen; note the air density inside the pseudoaneurysm signifying fistulous communication with the duodenum (blue arrow).
Figure: Figure 2: A Computed Tomogram (CT) Angiogram. Celiac trunk (black arrow), Left gastric artery (blue arrow), Splenic artery (purple arrow), Common hepatic artery (green arrow), Left hepatic artery (red arrow), Superior mesenteric artery (orange arrow), Accessory hepatic artery (white arrow). The accessory hepatic artery is arising from the superior mesenteric artery.
Disclosures: Azeem Khalid indicated no relevant financial relationships. Asad Ur Rehman indicated no relevant financial relationships. Muhammad Ahsan Asif indicated no relevant financial relationships. Muhammad Raffey Shabbir indicated no relevant financial relationships. Ibrar Atiq indicated no relevant financial relationships.
Azeem Khalid, MD1, Asad Ur Rehman, MD2, Muhammad Ahsan Asif, MBBS3, Muhammad Raffey Shabbir, MD4, Ibrar Atiq, MD5. P5233 - A Case of Fistula Formation Between Pseudoaneurysm of Hepatic Artery and Duodenum: A Rare Cause of Upper Gastrointestinal Bleeding (UGIB), ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")