Elmhurst Hospital Center / Icahn School of Medicine at Mount Sinai Queens, NY
Bibhuti Adhikari, MD1, Anastasia Novikov, MD1, Joshua Aron, MD2 1Elmhurst Hospital Center / Icahn School of Medicine at Mount Sinai, Queens, NY; 2Elmhurst Hospital Center / Icahn School of Medicine at Mount Sinai, New York, NY Introduction: Upper gastrointestinal bleeding (UGIB) is a common emergency, often caused by peptic ulcers, varices, or erosive gastritis. Vascular sources like visceral artery pseudoaneurysms (VAPA) are rare but potentially fatal. The inferior mesenteric artery (IMA) typically supplies the distal colon; its involvement in duodenal bleeding is exceedingly rare. We present a case of UGIB from an aberrant IMA pseudoaneurysm supplying the duodenum.
Case Description/
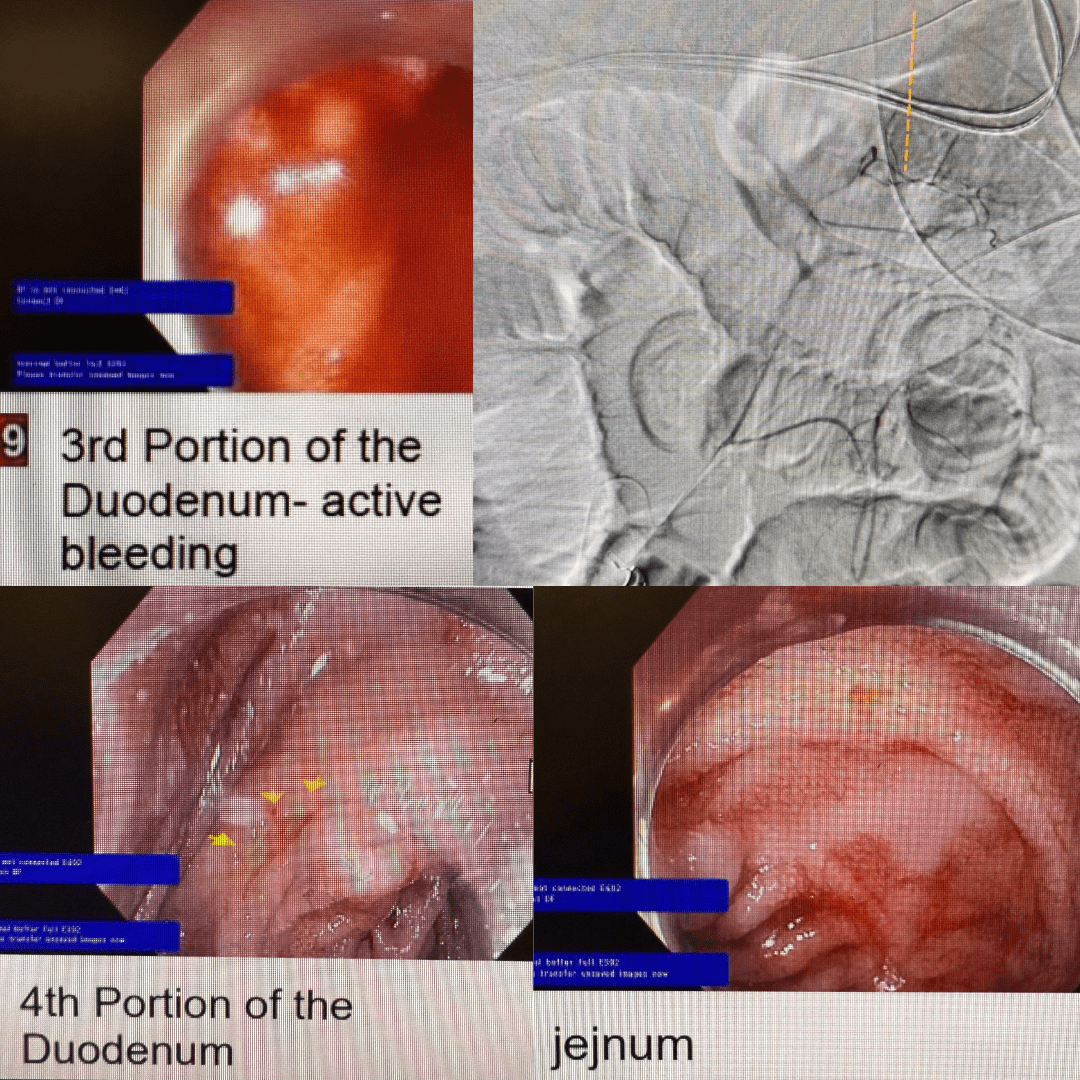
Methods: A 62-year-old male with no significant medical history presented with three days of melena and hematochezia, accompanied by dizziness, nausea, and cramping. On arrival, he was hypotensive (BP 88/53 mmHg), tachycardic (HR 102), and anemic (Hb 6.4 g/dL), and remained hemodynamically unstable despite receiving 7 units of PRBCs and 1 unit of FFP. A contrast-enhanced CT abdomen showed a subepithelial duodenal bulb lesion without evidence of active extravasation. Emergent EGD revealed a 1.5 cm submucosal lesion without active bleeding (likely a GIST), but massive active bleeding was noted in the third portion of the duodenum. All attempts at clot removal, including mechanical methods, were unsuccessful. Hemostatic spray was applied without success.
Given the location of the suspected pathology, the CT was re-reviewed with radiology, revealing an aberrant inferior mesenteric artery (IMA) supplying the third portion of the duodenum, with a pseudoaneurysm identified as the source of active bleeding. Interventional radiology (IR) angiography confirmed the bleeding pseudoaneurysm, and coil embolization of the lesion and its feeding vessel successfully achieved hemostasis without bowel compromise—a key concern prior to embolization.
A repeat endoscopic evaluation following IR embolization revealed an ulceration in the third portion of the duodenum.
Discussion: Pseudoaneurysms arise from full-thickness vessel wall disruption, often due to trauma, inflammation, or instrumentation. While the duodenum is normally supplied by celiac and SMA branches, rare variants like an aberrant IMA branch may contribute. Endoscopic therapy was limited by visualization challenges. CT angiography and IR intervention were key to diagnosis and management. This case highlights the need to consider vascular anomalies in refractory UGIB and the importance of multidisciplinary care.
Figure: IMA Pseudoaneurysm supplying the third portion of the duodenum
Disclosures: Bibhuti Adhikari indicated no relevant financial relationships. Anastasia Novikov indicated no relevant financial relationships. Joshua Aron indicated no relevant financial relationships.
Bibhuti Adhikari, MD1, Anastasia Novikov, MD1, Joshua Aron, MD2. P5227 - Unexpected Vascular Etiology of Upper GI Bleed: IMA Branch Pseudoaneurysm, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.