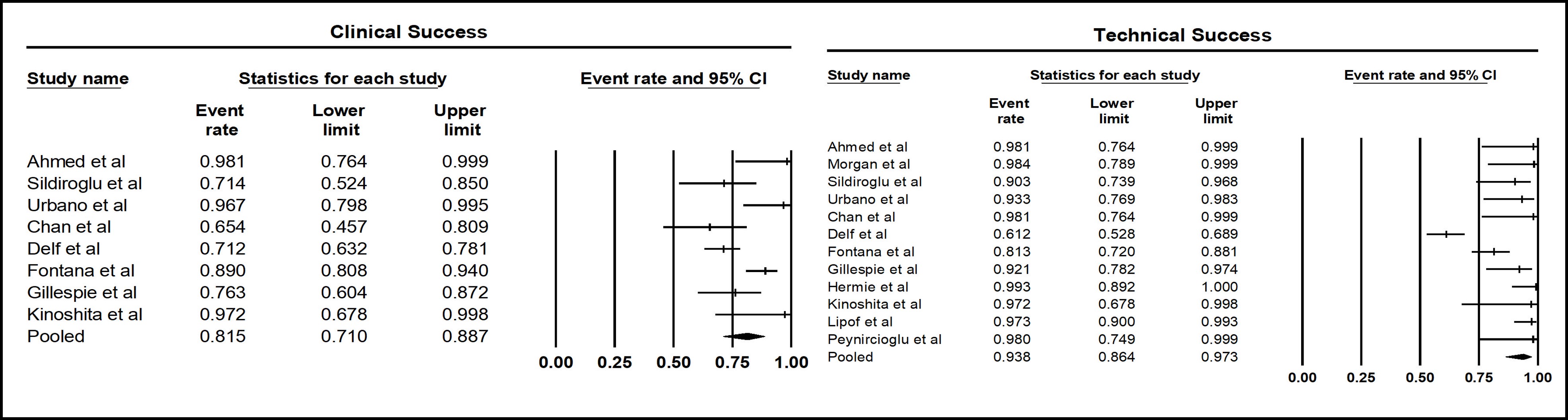
Sheza Malik, MD1, Marina Takawy, MD2, Umer Mukhtar, MD3, Vishali Moond, MD4, Babu P. Mohan, MD5, Douglas G. Adler, MD, FACG6 1Emory University, Atlanta, GA; 2Rochester Regional Health, Unity Hospital, Rochester, NY; 3Rochester General Hospital, Rochester, NY; 4Saint Peter's University Hospital/Robert Wood Johnson Medical School loc, New Brunswick, NJ; 5Orlando Gastroenterology PA, Orlando, FL; 6Center for Advanced Therapeutic (CATE), Centura Health, Porter Adventist Hospital, Peak Gastroenterology, Denver, CO Introduction: CTA (Computed Tomography Angiography) is a diagnostic tool widely used in the management of gastrointestinal bleeding. This study aims to evaluate the technical and clinical success rates of CTA embolization and assess the associated risks of rebleeding, re-embolization, surgery, endoscopy, and mortality. We analyze pooled data from various studies to determine the effectiveness of CTA in treating gastrointestinal bleeding and the factors influencing these outcomes. Methods: A systematic review and meta-analysis were conducted, including studies reporting on CTA outcomes in patients with gastrointestinal bleeding. The random effects model was employed to calculate pooled event rates, with 95% confidence intervals (CI) and I² statistics used to assess heterogeneity. P-values were calculated for significant differences across outcomes. Results: The pooled event rate for CTA embolization technical success was 93.8% (95% CI: 86.4%–97.3%; p< 0.001). Clinical success followed a similar trend, with a pooled rate of 81.5% (95% CI: 71.0%–88.7%; p< 0.001). However, the risk of rebleeding post-embolization was significant, with a pooled event rate of 19.3% (95% CI: 15.2-24.3; p< 0.05). The risk of re-embolization was 6.7% (95% CI: 4.0-11.0; p< 0.05), and the rate of patients requiring surgery was 10.0% (95% CI: 5.5-18.0; p< 0.05). The need for endoscopy after embolization occurred in 4.1% of cases (95% CI: 1.7-9.4; p< 0.05). The pooled mortality rate was 1.5% (95% CI: 1.07-2.0; p< 0.05). Discussion: CTA embolization demonstrates high technical and clinical success rates. However, the risk of rebleeding and the need for further interventions, such as re-embolization, surgery, and endoscopy, remain considerable. These findings underscore the importance of close monitoring and additional management strategies to optimize outcomes in gastrointestinal bleeding treatment.
Figure: Clinical and Technical Success Rate for CTA with Embolization in Patients with GI Bleed
Figure: Risk of Rebleed with CTA with Embolization in Patients with GI Bleed
Disclosures: Sheza Malik indicated no relevant financial relationships. Marina Takawy indicated no relevant financial relationships. Umer Mukhtar indicated no relevant financial relationships. Vishali Moond indicated no relevant financial relationships. Babu Mohan indicated no relevant financial relationships. Douglas Adler: Boston Scientific – Consultant.
Sheza Malik, MD1, Marina Takawy, MD2, Umer Mukhtar, MD3, Vishali Moond, MD4, Babu P. Mohan, MD5, Douglas G. Adler, MD, FACG6. P5207 - The Role of CTA Embolization in Managing Gastrointestinal Bleeding: A Comprehensive Review of Post-Embolization Risks, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.