Phoenixville Hospital - Tower Health Phoenixville, PA
Hatem Ahmed, MD1, Annapurna Korimilli, MD2 1Phoenixville Hospital - Tower Health, Phoenixville, PA; 2Penn Gastroenterology Limerick, Limerick, PA Introduction: Endometriosis classically involves pelvic structures, yet gastrointestinal extension is reported in only 3.8 – 37 % of cases and is usually serosal or muscular. True mucosal or submucosal disease is exceptionally uncommon and may masquerade as neoplasia, particularly in women with no prior diagnosis of endometriosis. We describe a rare polypoid presentation of colonic submucosal endometriosis detected incidentally during colonoscopy.
Case Description/
Methods: A 49-year-old woman (G2P2) with gastroesophageal reflux disease, hypertension, hyperlipidemia, and a remote hysterectomy for fibroids was evaluated for worsening generalized abdominal pain. She denied NSAID use and had recently stopped pantoprazole. Family history was notable for a maternal grandmother with colorectal cancer. Vitals, physical examination, and laboratory studies—including hemoglobin (13 g/dL), ferritin (107 ng/mL), and iron indices—were unremarkable. Esophagogastroduodenoscopy showed Grade B esophagitis and mild antral gastritis. Colonoscopy revealed diverticulosis and a solitary 18 mm sessile polyp located 30 cm from the anal verge, which was completely removed with a hot snare and clipped. Two small (2 mm) sessile serrated lesions were also excised. Histology of the 18 mm lesion demonstrated submucosal endometrial glands and stroma with rare mucosal involvement. Immunohistochemistry was positive for estrogen receptor, PAX8, and stromal CD10, but negative for CDX2 and CK20, confirming ectopic endometrium. The remaining polyps were benign sessile serrated lesions without dysplasia. The patient had no clinical or imaging evidence of residual or extra-intestinal endometriosis. Discussion: Submucosal colonic endometriosis is an extraordinary mimic of colorectal neoplasia. In women of reproductive age, even those with prior hysterectomy but no documented endometriosis, endoscopic polypoid lesions can conceal ectopic endometrial tissue. Awareness of this entity and appropriate use of immunohistochemistry are essential to avoid misdiagnosis and to guide appropriate surveillance and management.
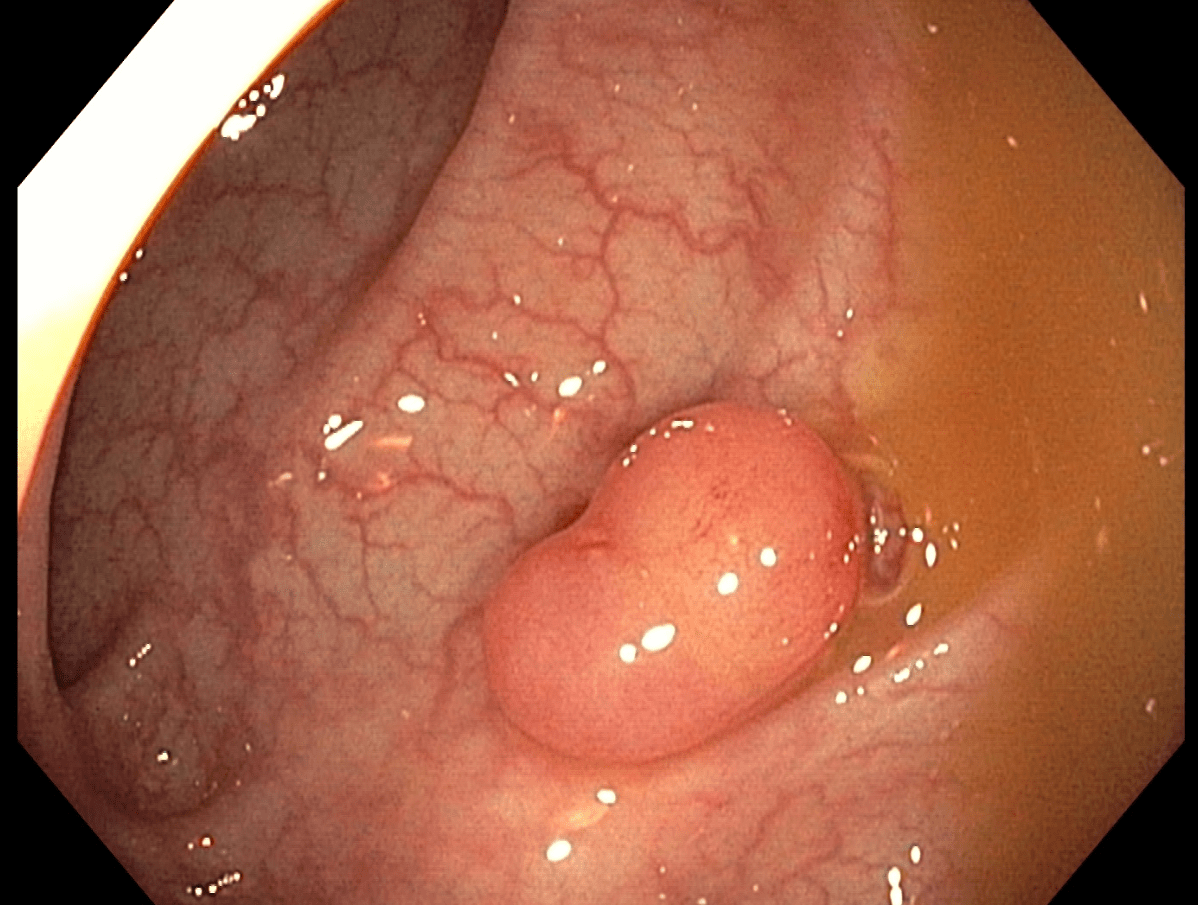
Figure: Figure 1. Colonoscopic view of the 18 mm sessile polyp located 30 cm from the anal verge in the sigmoid colon; histology later confirmed submucosal endometriosis masquerading as a benign-appearing polyp
Disclosures: Hatem Ahmed indicated no relevant financial relationships. Annapurna Korimilli indicated no relevant financial relationships.
Hatem Ahmed, MD1, Annapurna Korimilli, MD2. P5177 - Colonic Submucosal Endometriosis: A Case Report of a Diagnostic Dilemma in the Absence of Known Endometriosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.