Robert Wood Johnson Medical School, Rutgers University New Brunswick, NJ
Award: ACG Presidential Poster Award
Shivani Patel, MD1, Ankoor Patel, MD1, Courtney Smalley, BS2, Steven Brant, MD1 1Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ; 2Rutgers Robert Wood Johnson University Hospital, New Brunswick, NJ Introduction: Caustic ingestions are a common cause for injuries to the upper gastrointestinal tract, most notable the esophagus and stomach. We report a case of caustic injury to the upper GI tract following ingestion of potassium thiocyanate, an occurrence which has not been previously reported.
Case Description/
Methods: A 48-year-old female with a history of depression presented following ingestion of potassium thiocyanate approximately two hours prior to arrival. She had multiple episodes of hematemesis and hematochezia. On exam, she was lethargic with evidence of perioral dried blood, hyperactive bowel sounds, and dark red blood on rectal exam. Labs showed leukocytosis, anemia, hyperkalemia, and worsening acidosis. CT findings demonstrated mild esophageal wall thickening and edema, severe diffuse wall thickening of the stomach, duodenum, and majority of the jejunum with fat stranding and edema. The patient was started on IV PPI twice daily. EGD showed Zargar Caustic Ingestion Injury Grade 1 in the proximal esophagus, Grade 2a at the distal 3 cm of the esophagus, and Grade 3a gastritis with diffuse severe mucosal changes with areas of black discoloration and ulceration along entire stomach from both the greater and lesser curvature to antrum/prepyloric region (Figure). Due to concern for extensive and transmural necrosis of the stomach, the patient underwent immediate exploratory laparotomy revealing a thickened but nonthreatened stomach with an ulcer visualized at the GE junction on the posterior stomach, threatened 1 cm D2 segment of the duodenum, and thickened and scattered petechiae of the first 60 cm of the jejunum without evidence of overt necrosis. The colon was healthy appearing. The abdomen was left open and the patient returned to the OR after 48 hours for abdominal washout and closure. At the time, no further progression of ischemia or necrosis of bowel was noted. On day 18, the patient underwent an esophagram, showing no esophageal leakage and mild delayed contrast transit to the stomach and mild distal esophagitis, gastritis, and duodenitis. The NG tube was removed on day 19, and the patient subsequently tolerated an oral diet and was discharged on day 24. Discussion: We present the first case of caustic injury to the upper GI tract following ingestion of potassium thiocyanate. Our case emphasizes the importance of immediate endoscopic evaluation to determine the severity of tissue injury in order to determine treatment options and predict prognosis.
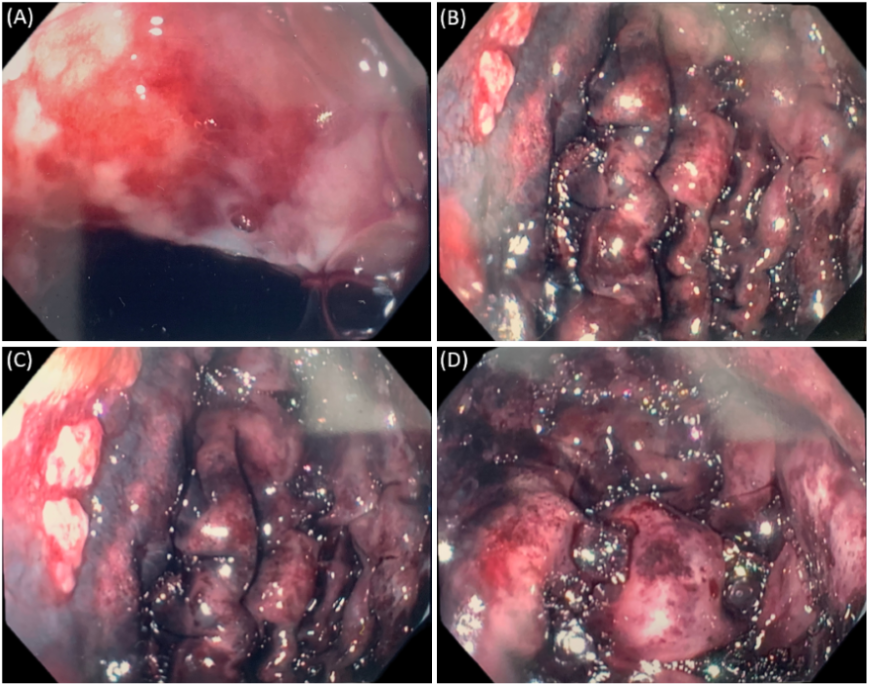
Figure: Figure 1. (A) Evidence of superficial ulceration, erosions, friability, and blistering in the distal esophagus (3cm from the GEJ), classified as Zargar Grade 2a. (B, C, D) Evidence of scattered areas of necrosis as evidenced by black discoloration along the greater curvature of the stomach, classified as Zargar Grade 3a.
Disclosures: Shivani Patel indicated no relevant financial relationships. Ankoor Patel indicated no relevant financial relationships. Courtney Smalley indicated no relevant financial relationships. Steven Brant indicated no relevant financial relationships.
Shivani Patel, MD1, Ankoor Patel, MD1, Courtney Smalley, BS2, Steven Brant, MD1. P5176 - A Case of Caustic Ingestion With Potassium Thiocyanate, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.