Washington State University Elson S. Floyd School of Medicine Spokane, WA
Evelyn H.. Rowe, BS1, Lauren Duffy, BS2, Renee Umbdenstock, MD3, David H. Johnson, MD4 1Washington State University Elson S. Floyd School of Medicine, Spokane, WA; 2Washington State University Elson S. Floyd School of Medicine, Seattle, WA; 3Anesthesia Associates of Coeur d’Alene, Coeur d'Alene, ID; 4Kootenai Clinic Gastroenterology and Endoscopy, Coeur d'Alene, ID Introduction: We report the case of a 60-year-old female with esophageal obstruction due to denture adhesive. She has a medical history of end-stage renal disease on dialysis, ileostomy, and edentulism. She presented to the Emergency Department (ED) with nausea, vomiting, and abdominal pain. She received conservative treatment with ondansetron, intravenous fluids and improved sufficiently for dismissal home. Later that day she returned to the ED due to persistent oral intolerance. Computed Tomography (CT) was obtained showing bubbly mixed density contrast material and annular mural thickening of the distal esophagus with a thin column of liquid across the gastroesophageal junction consistent with a food impaction.
Case Description/
Methods: Based on the CT results, Gastroenterology was consulted for urgent upper endoscopy. Endoscopic visualization revealed what appeared to be superficial peeling in the mid esophagus and dense cake-like adherent material in the distal esophagus. Unusually colored turquoise fluid was noted in the stomach. The procedure was made difficult by the scope sticking or adhering to the esophageal wall which required careful torquing and gentle withdrawal followed by copious lubrication of the insertion tube before re-insertion. Removal of some material with washing the esophagus revealed normal underlying mucosa. Due to dense adhesion of the material and clogging of the suction channel only a modest amount of the material could be removed.
It was noted during pre-procedural consent that she was extremely self-conscious about having dentures. Following the procedure, she disclosed frequent use of copious amounts of denture adhesive paste in an attempt to avoid embarrassment from denture movement. Given the history and endoscopic procedure, the diagnosis of esophageal obstruction due to denture adhesive was made. Esophagitis dissecans superficialis was also considered. Discussion: The patient was recommended to refrain from denture and adhesive use and to drink one can of diet cola daily. Follow-up endoscopy 11 days later showed complete resolution of the previous visual abnormalities and normal esophageal mucosa. No dysphagia remained. This case highlights a rare cause of esophageal obstruction and the risk of excessive denture adhesive use. The acidic and carbonated properties of diet cola can enhance swallowing and, in some cases, break down adhesive components. For our patient diet cola was an effective treatment modality and completely resolved her symptoms.
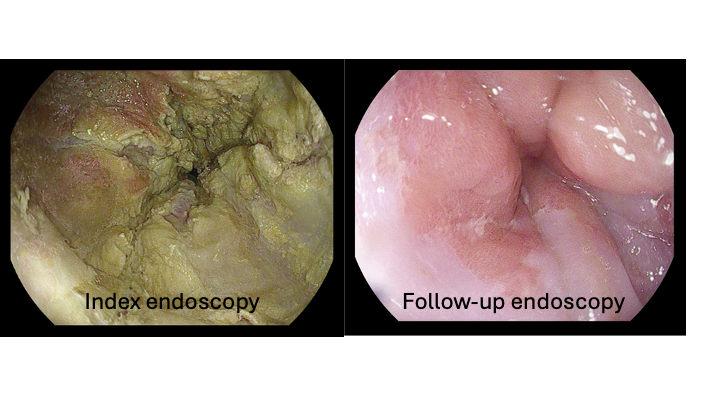
Figure: Figure 1. Index endoscopy with dense caking of material in the distal esophagus and follow-up endoscopy 11 days later showing absence of foreign material and normal mucosa.
Disclosures: Evelyn Rowe indicated no relevant financial relationships. Lauren Duffy indicated no relevant financial relationships. Renee Umbdenstock indicated no relevant financial relationships. David Johnson: Abbvie – Speakers Bureau. Bristol Myers Squibb – Speakers Bureau. Takeda – Advisory Committee/Board Member.
Evelyn H.. Rowe, BS1, Lauren Duffy, BS2, Renee Umbdenstock, MD3, David H. Johnson, MD4. P5175 - Esophageal Obstruction due to Denture Adhesive Masquerading as a Food Bolus, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")