Momin Masroor, MD1, Suhail Sidhu, MD1, Bryant Le, MD1, Shoujit Banerjee, MD1, Andy Lin, MD1, Frances Dang, MD, MSc2, Peter H. Nguyen, MD3, Jason Samarasena, MD, MBA, FACG1 1University of California Irvine, Orange, CA; 2University of California Irvine, Irvine, CA; 3University of California Irvine Health, Orange, CA Introduction: Kaposi’s Sarcoma is a soft tissue malignancy that is caused by HHV-8 infection in immunocompromised patients and is an AIDS-defining illness. Kaposi’s Sarcoma typically involves diffuse skin and in more advanced cases, visceral organ involvement including that of the GI tract. This case describes how endoscopic guided tissue sampling informed decision making for definitive management of visceral Kaposi’s Sarcoma.
Case Description/
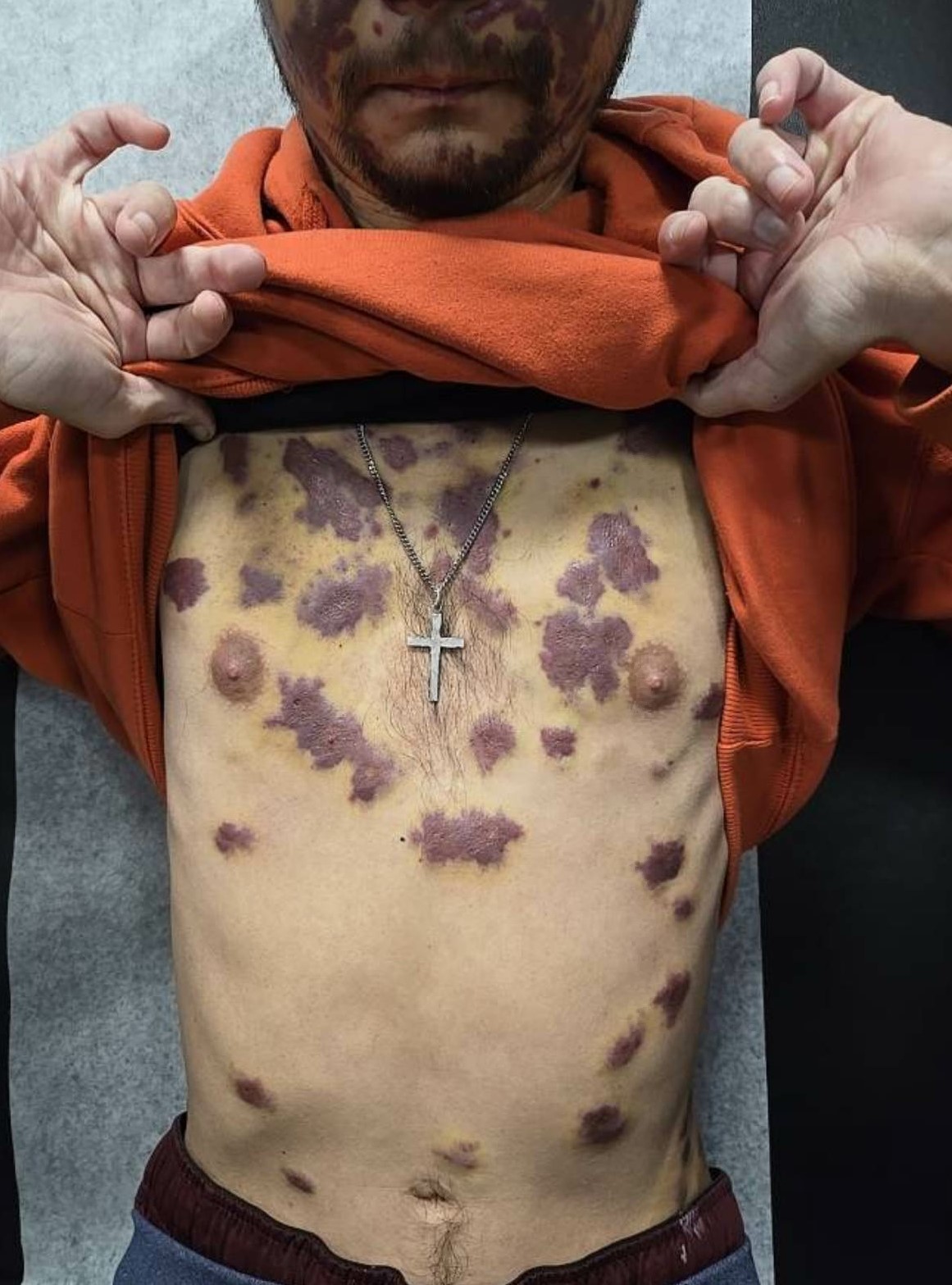
Methods: 34 year old male with no known medical history presented with worsening rash on face and body and swelling of the eyelids. Patient reported that his rash began with a small lesion next to his eye eight months prior but had steadily been worsening (Figure 1). He was found to be HIV antibody positive on admission with a CD4 count of fifty. HHV-8 immunostain was positive on dermatologic punch biopsy which supported a diagnosis of Kaposi’s Sarcoma. He underwent a bronchoscopy with bronchoalveolar lavage positive for PJP and CMV, but not HHV-8. Given concern for disseminated Kaposi’s Sarcoma, he was started on Doxarubicin and antiretroviral treatment for HIV. GI was consulted to evaluate concern of visceral involvement and if he would require additional chemotherapy outpatient. EGD demonstrated two raised erythematous nodular appearing lesions at the GE junction, measuring 5 mm in size (HHV-8 immunostain positive) (Figure 2). Colonoscopy demonstrated scattered patchy erythema with mild superficial ulceration in the rectum (HHV-8 immunostain positive) (Figure 2). He improved with initiation of systemic Doxarubicin and anti-retroviral therapy and discharged with close outpatient oncology and infectious disease follow-up for consideration of further treatment given visceral involvement. Discussion: The mainstay treatment for AIDS-related Kaposi’s Sarcoma involves anti-retroviral therapy. In cases in which there is visceral involvement, systemic chemotherapy should be considered. This case highlights the importance of gastrointestinal endoscopy to guide management of AIDS-related Kaposi’s Sarcoma. Further research is warranted to determine the optimal timing and indications for endoscopic evaluation in patients with cutaneous Kaposi’s Sarcoma.
Figure: Figure 1: Extensive dermatologic involvement of Kaposi’s Sarcoma over his trunk and face.
Figure: Figure 2: EGD demonstrating nodular erythematous lesion at the GE junction which was positive for HHV-8 immunostain (2A). Colonoscopy demonstrating patchy erythema with superficial ulceration of the rectum which was positive for HHV-8 immunostain (2B).
Disclosures: Momin Masroor indicated no relevant financial relationships. Suhail Sidhu indicated no relevant financial relationships. Bryant Le indicated no relevant financial relationships. Shoujit Banerjee indicated no relevant financial relationships. Andy Lin indicated no relevant financial relationships. Frances Dang: Cook Medical – Speaker. Peter Nguyen indicated no relevant financial relationships. Jason Samarasena: Applied Medical – Consultant. Boston Scientific – Consultant. Cook Medical – Consultant. Neptune Medical – Consultant. Olympus – Consultant.
Momin Masroor, MD1, Suhail Sidhu, MD1, Bryant Le, MD1, Shoujit Banerjee, MD1, Andy Lin, MD1, Frances Dang, MD, MSc2, Peter H. Nguyen, MD3, Jason Samarasena, MD, MBA, FACG1. P5173 - Cutaneous Clues, Visceral Truths: Uncovering Kaposi’s Sarcoma in the GI Tract, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.