Agustin Gavidia Rosario, MD1, Mohammed Abusuliman, MD2, Diana Jomaa-Rteil, MD1, Sumair Ahmad, MD1 1Henry Ford Health, Detroit, MI; 2Henry Ford Hospital, Detroit, MI Introduction: Mycobacterium avium complex (MAC) and cytomegalovirus (CMV) are opportunistic infections commonly encountered in immunocompromised individuals and can sometimes be life-treatening. While both infections can involve the gastrointestinal tract, their simultaneous occurrence is rare and literature review has revealed only 1 prior documented case. Our case highlights the diagnostic challenges posed by co-infections of MAC duodenitis and CMV esophagitis in an advanced HIV patient and the importance of prompt recognition.
Case Description/
Methods: A 43-year-old trans-female with advanced HIV (CD4 count 22 cells/µL, undetectable viral load), complicated by disseminated MAC with colon involvement, presented with 2 weeks of nausea, vomiting, dysphagia, and failure to thrive. Empiric treatment with fluconazole and enteric nutrition via a Dobhoff feeding tube led to mild symptomatic improvement. She then had an esophagogastroduodenoscopy (EGD) done that was significant for diffuse edema, white patchy granularity, nodularity, and blunting and scalloping of the duodenal folds, erythematous gastric mucosa, and a normal esophagus. Histopathology confirmed CMV inclusions in the esophagus and Mycobacterium avium complex in the duodenum. The patient continued to improve with appropriate antimicrobial therapy for both infections. Discussion: This case highlights an unusual co-infection infection with MAC duodenitis and CMV esophagitis in an immunocompromised HIV patient. Although each infection typically presents independently, their co-occurrence, in this case, presents a diagnostic challenge, requiring a high index of suspicion. Although physical examination and history are key for diagnosis, physicians should be highly suspicious of these infections, especially as early endoscopic interventions help confirm the diagnosis.
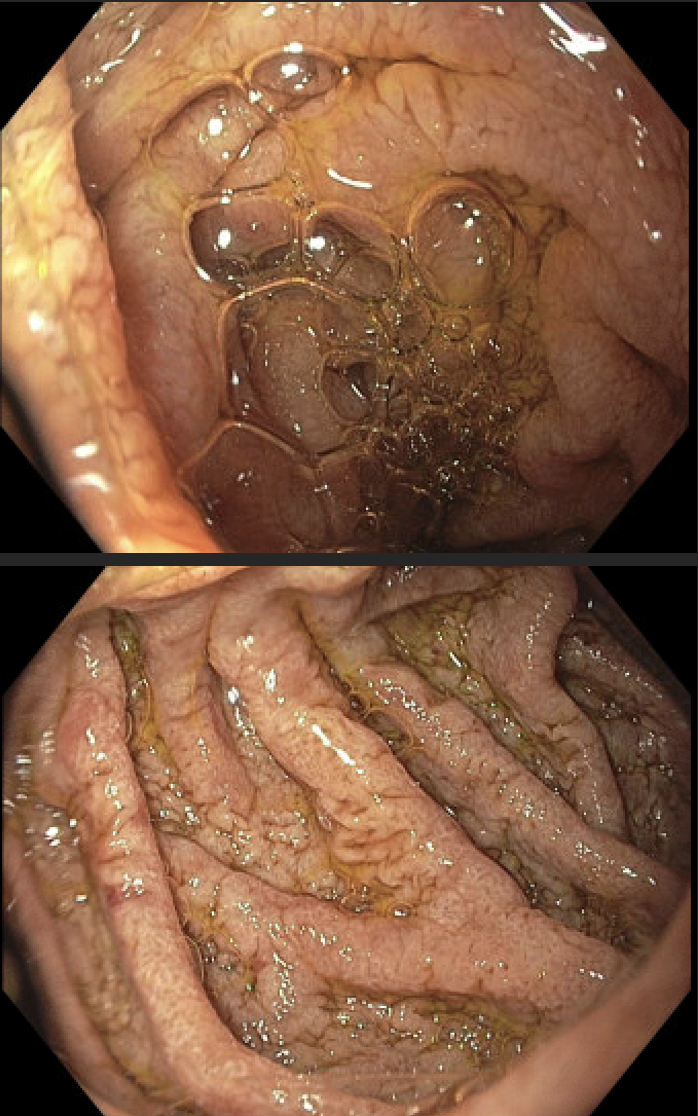
Figure: Image 1: EGD showing duodenum with diffuse edema , white patchy granularity, nodularity, blunting and scalloping of the duodenal folds.
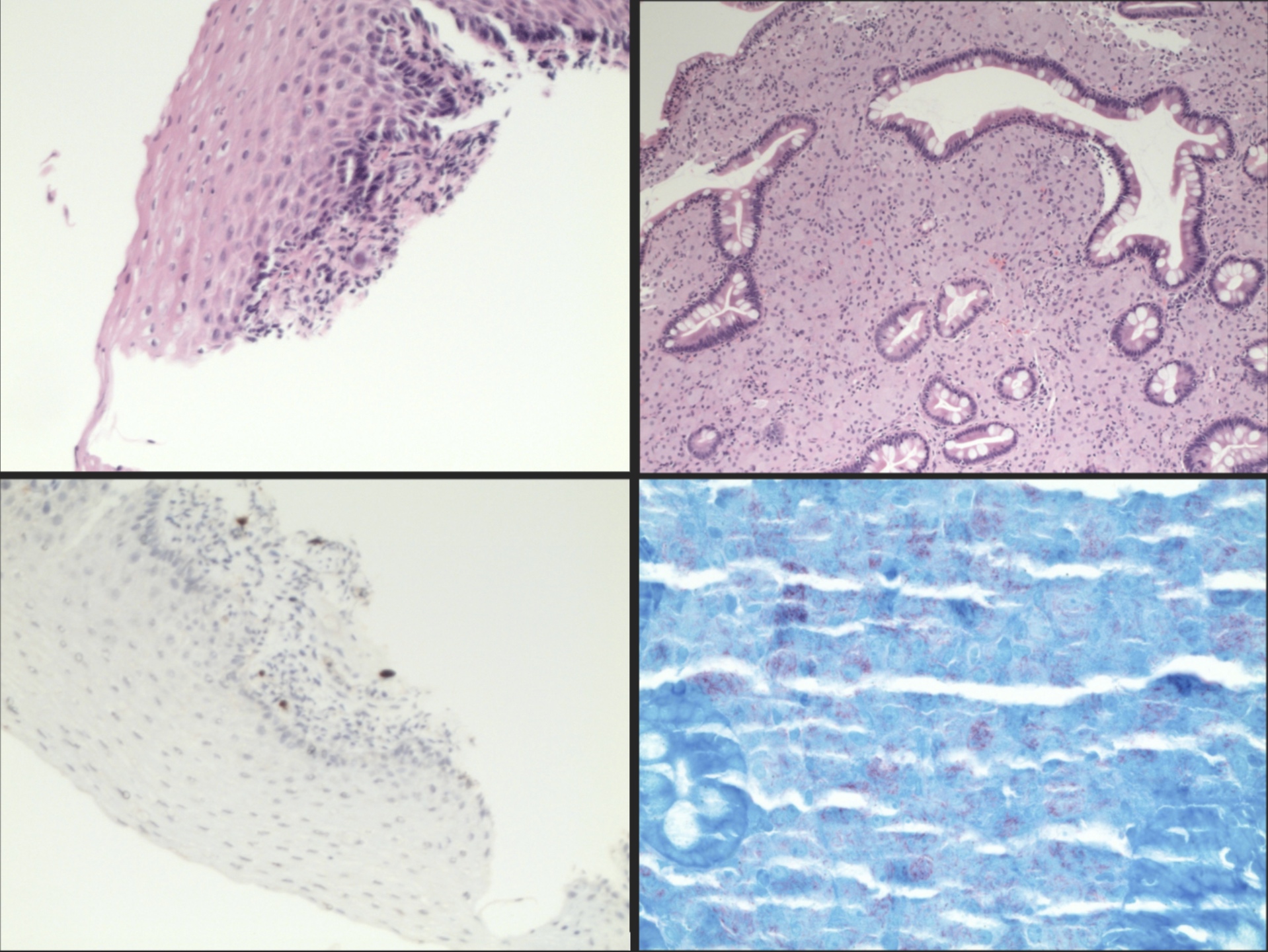
Figure: Image 2: Esophagus with CMV inclussions (top right), CMV positive stain in the inclusions (bottom right), duodenal mucosa with lamina propria packed with foamy histiocytes (top left) and duodenal mucosa with AFB stain highlighting red color bacilli (bottom right).
Disclosures: Agustin Gavidia Rosario indicated no relevant financial relationships. Mohammed Abusuliman indicated no relevant financial relationships. Diana Jomaa-Rteil indicated no relevant financial relationships. Sumair Ahmad indicated no relevant financial relationships.
Agustin Gavidia Rosario, MD1, Mohammed Abusuliman, MD2, Diana Jomaa-Rteil, MD1, Sumair Ahmad, MD1. P5164 - Mycobacterium Avium Complex (MAC) Duodenitis and Cytomegalovirus (CMV) Esophagitis Coinfection in an Advanced HIV Patient: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.