University of Colorado Anschutz Medical Campus Aurora, CO
Malique Delbrune, MD1, Corrine Camp, MD1, Anna Holcomb, DO2, Mohammad Bilal, MD, FACG3 1University of Colorado Anschutz Medical Campus, Aurora, CO; 2University of New England College of Osteopathic Medicine, New England, ME; 3University of Colorado Anschutz Medical Campus, Denver, CO Introduction: Hematemesis with hemodynamic instability is a medical emergency requiring immediate intervention. While the differential for source of bleeding is broad, there typically can be an educated prediction of likely sources based on a patient’s history. There are however times where an unanticipated culprit is discovered. We describe a patient with hematemesis who underwent esophagogastroduodenoscopy (EGD) found to have a duodenal mass secondary to an undiagnosed metastatic teratoma.
Case Description/
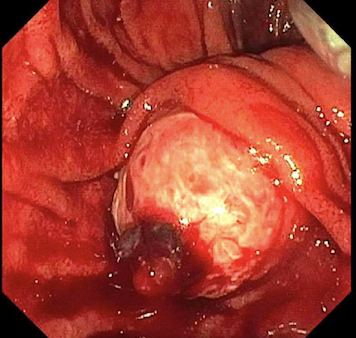
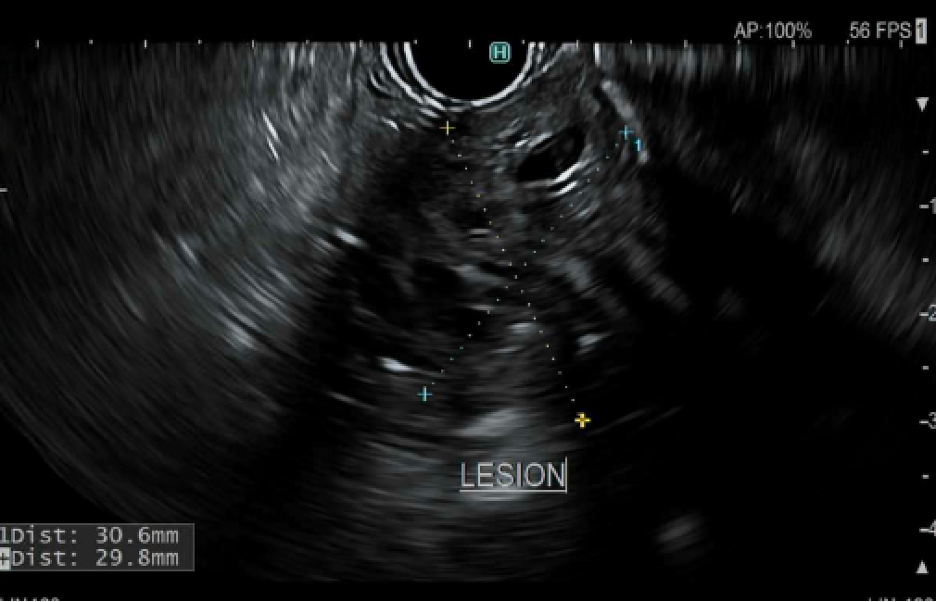
Methods: A 44-year-old male with past medical history of alcohol use disorder and prior infection with helicobacter pylori treated with antibiotics, had experienced two days of abdominal pain with hematemesis and melena. Physical exam was notable for tachycardia and laboratory data revealed anemia hemoglobin of 8.7 g/dL. EGD was performed and demonstrated a mass with active bleeding from a visible vessel in the second portion of the duodenum near the major papilla (Figure A). The vessel was cauterized with cessation of bleeding and biopsies obtained were positive for helicobacter pylori. Given the size and on evaluation there was concern for further depth of invasion cross sectional imaging was obtained. Computed tomography revealed a heterogenous right testicular mass measuring 8.4cm, concerning for a primary testicular cancer, as well as a large necrotic conglomerate of retroperitoneal pericaval lymph nodes at the level of the duodenum with likely invasion, suspicious for metastatic disease. Endoscopic ultrasound showed a 32mm by 39mm heterogenous duodenal mass with poorly defined borders sparing the ampulla (Figure B). Fine need biopsy was performed which showed areas of keratinizing squamous type mucosa on histology. Fluorescence in situ hybridization (FISH) was positive for isochrome 12p, supporting diagnosis of metastatic mature cystic teratoma. Orchiectomy was subsequently performed, and patient was treated with etoposide and cisplatin. Restaging scan after second chemotherapy cycle demonstrated a decrease in retroperitoneal nodal mass. Discussion: Gastrointestinal metastases are seen in a handful of germ cell tumors of the testes. The most common sites of metastases for testicular cancers such as teratomas are brain, liver, and lungs. Metastasis to the duodenum is exceedingly rare. This case highlights a rare and abnormal presentation of gastrointestinal symptoms due to an uncommon metastatic disease source.
Figure: Figure A. Duodenal mass with active bleeding from visible vessel
Figure: Figure B. Endoscopic ultrasound exam of duodenal mass.
Disclosures: Malique Delbrune indicated no relevant financial relationships. Corrine Camp indicated no relevant financial relationships. Anna Holcomb indicated no relevant financial relationships. Mohammad Bilal: Boston Scientific – Consultant. Cook endoscopy – Paid speaker. Steris Endoscopy – Consultant.
Malique Delbrune, MD1, Corrine Camp, MD1, Anna Holcomb, DO2, Mohammad Bilal, MD, FACG3. P5153 - Metastatic Teratoma Resulting in Upper Gastrointesinal Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")