Brown University / Rhode Island Hospital Providence, RI
Andrew L. Petrou, MD1, Temitope Omoladun-Tijani, MD, MPH1, Priya Kumari Maheshwari, MD2, Jason Ferreira, MD3 1Brown University / Rhode Island Hospital, Providence, RI; 2University of Central Florida, HCA Healthcare GME, Pensacola, FL; 3University Gastroenterology, Providence, RI Introduction: Rectovesical fistulas (RVFs) are abnormal connections between the rectum and the urinary bladder. Although rare, RVFs can present with a spectrum of urinary and gastrointestinal symptoms, including pneumaturia, fecaluria, and recurrent urinary tract infections. Here we describe a rare presentation of a rectovesical fistula allowing direct passage of a colonoscope into the bladder. Notably, the fistulous tract enabled transrectal endoscopic visualization and biopsy of a suspicious bladder mass.
Case Description/
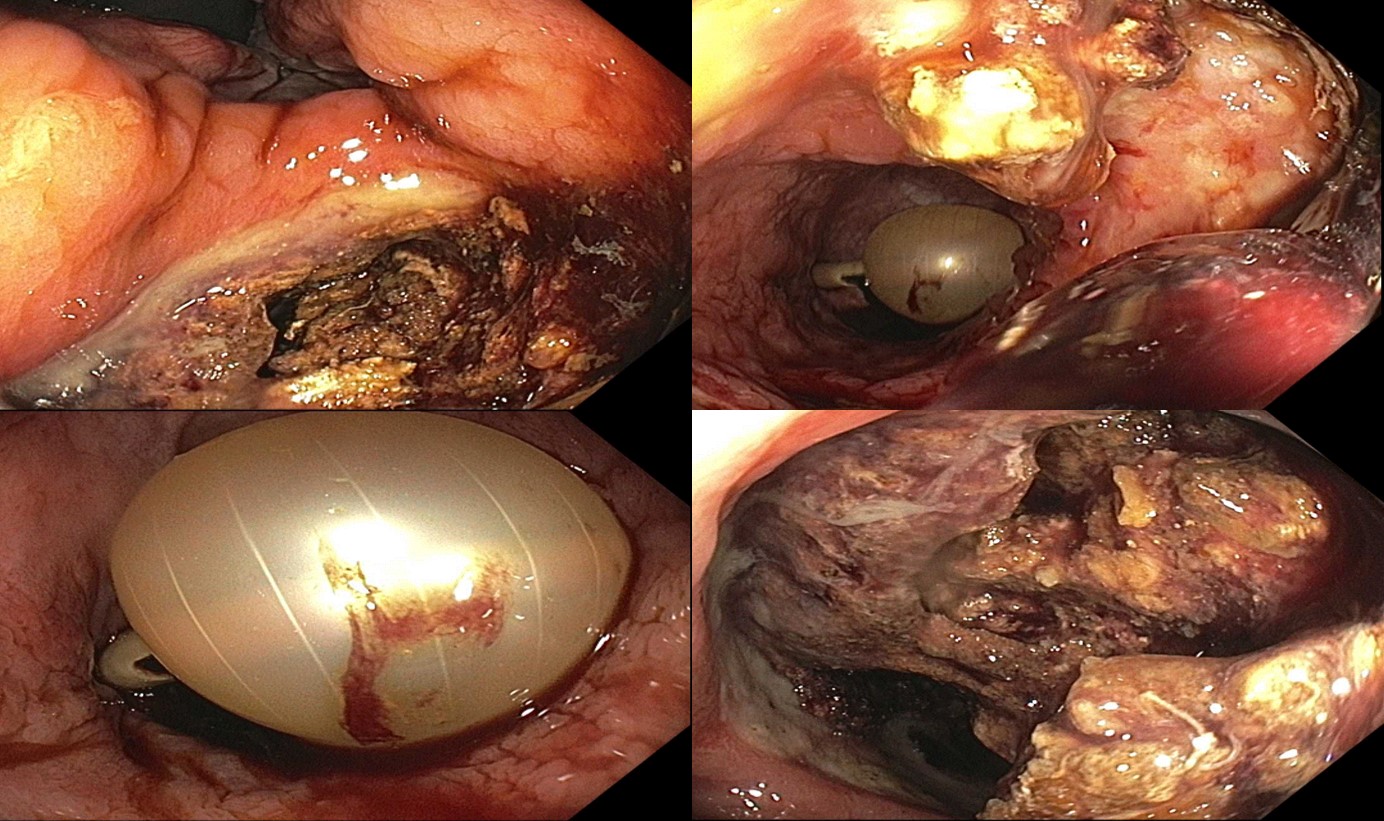
Methods: A 79-year-old male with a past medical history of prostate cancer treated with radical retropubic prostatectomy and rectourethral fistula with suprapubic catheter placement presented to the hospital for persistent rectal bleeding and fecaluria. Physical exam was unrevealing and the suprapubic catheter site showed no signs of surrounding erythema. Notable labs included hemoglobin 11.3 g/dL compared to a baseline of 12.0 g/dL, alkaline phosphatase of 121 IU/L. Computed tomography angiography of the abdomen and pelvis showed known RVF and new bladder wall thickening. The gastroenterology team was consulted, and colonoscopy was recommended. During the procedure, a large fistula in the rectum connecting to the bladder was identified. The colonoscope traversed the fistula, and a large bladder mass was visualized, appearing to be the likely cause of the fistulization. Bleeding was noted within the bladder, likely related to the mass, and biopsies were taken for histology. Interestingly, the histology was negative for malignancy, and the patient was referred to colorectal surgery for fistula management. Discussion: Endoscopic access to the bladder through an RVF during colonoscopy is rare. In our case, the colonoscope was advanced through the fistulous tract, providing direct visualization of the bladder mucosa and biopsy of a suspicious lesion. While this route of access is unconventional, it highlights the potential utility of existing fistulous tracts for diagnostic purposes. In this situation, the cause of the bladder mass and fistula were likely related to prior radiation therapy that he had received in the setting of his prostate cancer. This case emphasizes the importance of maintaining vigilance during endoscopic procedures, particularly in patients with known or suspected pelvic fistulas, and showcases how an unexpected route can provide valuable diagnostic insights.
Figure: Figure 1. A large rectovesical fistula with scope traversal, revealing a suspected bladder mass with bleeding and a visualized suprapubic tube balloon. Biopsies of the suspected tumor were taken with cold forceps for histology.
Disclosures: Andrew Petrou indicated no relevant financial relationships. Temitope Omoladun-Tijani indicated no relevant financial relationships. Priya Kumari Maheshwari indicated no relevant financial relationships. Jason Ferreira indicated no relevant financial relationships.
Andrew L. Petrou, MD1, Temitope Omoladun-Tijani, MD, MPH1, Priya Kumari Maheshwari, MD2, Jason Ferreira, MD3. P5147 - An Unintended Route: Biopsy of a Bladder Mass During Colonoscopy via a Rectovesical Fistula, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")